
ADA 2026
Summer's hottest obesity & diabetes conference

Disclaimer: This newsletter is for educational and informational purposes only and does not constitute medical, investment, or financial advice, nor does it establish a provider-patient relationship. Content may include forward-looking statements and discussions of investigational therapeutic candidates that are not FDA/EMA approved; their safety and efficacy remain unestablished and clinical outcomes are unpredictable. While we strive for accuracy, all information is provided as is without guarantees. This newsletter is independent, and the author holds no financial positions in the companies mentioned nor receives third-party compensation for this coverage. Please find a complete version of our disclaimers at the bottom of this article and on our About page.

Press ⬇️ to go down to a section and ⬆️ to go back up to the Table of Contents
Table of Contents
The American Diabetes Association (ADA) 86th Scientific Sessions, held in New Orleans, Louisiana, from June 5–8, 2026, served as the premier global stage for groundbreaking research, clinical advances, and therapeutic shifts in diabetes care, obesity management, and metabolic health. Bringing together tens of thousands of clinicians, scientists, and industry leaders from around the world, the 2026 conference marked a definitive turning point in metabolic medicine. Unsurprisingly, the overarching theme of this year’s sessions focused on next-generation obesity/diabetes therapies.
This week, we discuss selected ADA 2026 datasets for:
Injectable Obesity Medicines
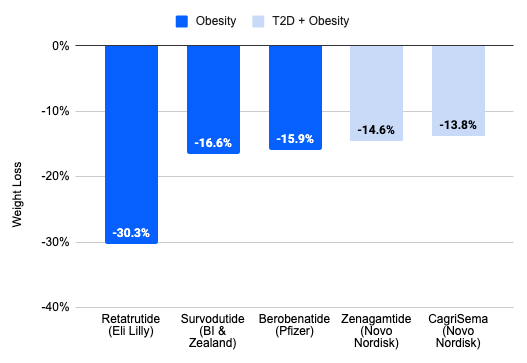
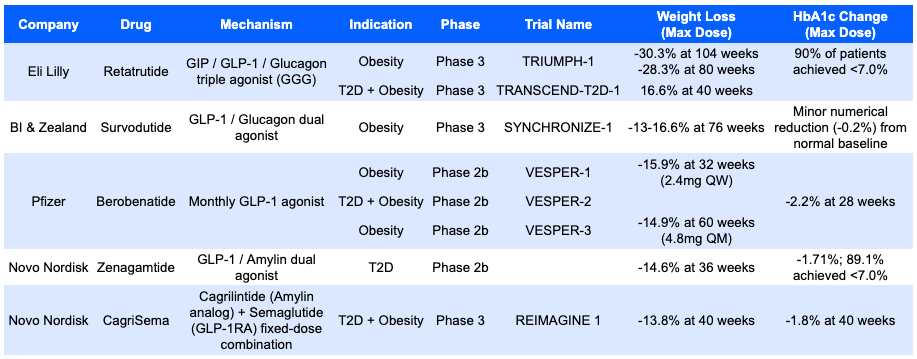
The absolute ceiling for weight loss at the conference was established by Eli Lilly’s retatrutide, a GIP/GLP-1/Glucagon triple receptor agonist (GGG). In the Phase 3 TRIUMPH-1 trial for non-diabetic obesity, retatrutide achieved historic, deep weight reductions of -28.3% at 80 weeks and -30.3% at 104 weeks. In the parallel Phase 3 TRANSCEND-T2D-1 trial evaluating a comorbid T2D population, the drug drove a 16.6% weight loss at 40 weeks. On the glycemic front, it allowed 90% of patients to cross the finishing line of an HbA1c < 7.0%.
Boehringer Ingelheim & Zealand Pharma countered with survodutide, a dual GLP-1/Glucagon receptor agonist. In the Phase 3 SYNCHRONIZE-1 trial for obesity, survodutide demonstrated a robust weight loss profile of -13-16.6% at 76 weeks. While it showed a minor numerical HbA1c drop of -0.2% from a normal baseline, the clinical focus of its dual-agonist mechanism heavily emphasized fat quality reduction rather than pure glucose lowering.
Pfizer utilized its Phase 2b VESPER program to showcase berobenatide, an investigational ultra-long-acting GLP-1 receptor agonist explicitly designed to challenge the industry’s standard weekly injection paradigm by evaluating both weekly and monthly regimens. The VESPER-1 trial evaluated a once-weekly (QW) subcutaneous dose, reaching a non-placebo-adjusted weight reduction of -15.9% at 32 weeks at the 2.4mg dose level. The VESPER-2 trial proved its glucose-lowering capabilities in a combined T2D and obesity population, delivering a strong -2.2% reduction in HbA1c at 28 weeks. The pivotal proof-of-concept came from the VESPER-3 obesity trial. By testing a once monthly (QM) maintenance strategy, Pfizer proved that patients transitioning to a 4.8mg once-monthly shot could successfully maintain their trajectory, clocking a -14.9% weight loss at 60 weeks without a plateau.
Novo Nordisk focused its presentations on leveraging the combination of amylin and GLP-1 pathways, showcasing two distinct molecular approaches to maximize metabolic control. In a Phase 2b dose-finding trial for type 2 diabetes, Zenagamtide (single-molecule GLP-1/Amylin dual agonist) turned heads by achieving a -14.6% weight reduction in just 36 weeks. This was paired with a -1.71% reduction in HbA1c, with 89.1% of patients achieving the target threshold of < 7.0%. Novo also presented Phase 3 data for CagriSema, a co-formulation of the amylin analog cagrilintide and semaglutide. In the REIMAGINE 1 trial (evaluating adults with T2D and obesity), the fixed-dose combo met its primary and secondary endpoints simultaneously, demonstrating a -13.8% weight loss alongside a -1.8% drop in HbA1c at 40 weeks.
Oral Obesity Medicines
The data from the oral medicine table maps out a fiercely competitive, small-molecule injectable to oral shift presented at ADA 2026. The readouts demonstrate that oral GLP-1 receptor agonists are attempting to close the efficacy gap with injectables, focusing heavily on maximizing convenience while maintaining glycemic control and weight loss.
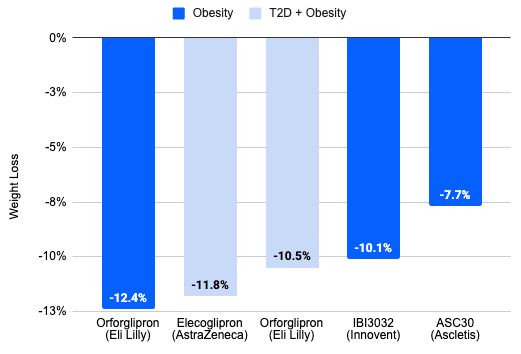
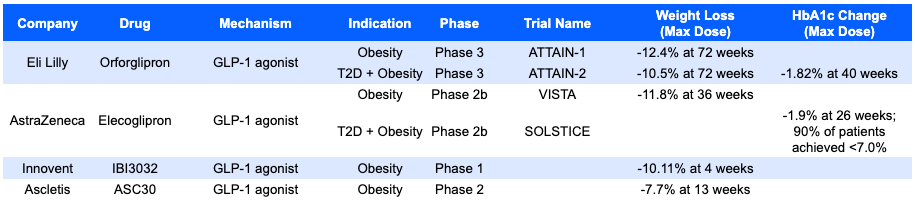
Eli Lilly anchored the oral small-molecule landscape with comprehensive Phase 3 data from its highly anticipated ATTAIN clinical trial program for orforglipron. In the Phase 3 ATTAIN-1 trial targeting adults with obesity, the daily pill demonstrated strong, sustained efficacy, driving a -12.4% weight loss at 72 weeks at the maximum dose. In the parallel ATTAIN-2 trial, orforglipron showed impressive dual efficacy in a historically harder-to-treat diabetic population. It delivered a ‒10.5% weight loss at 72 weeks, closely mirrored by a substantial -1.82% drop in HbA1c recorded at the 40-week milestone.
AstraZeneca emerged as a primary challenger in the oral small-molecule sector, showcasing mid-to-late stage data from its elecoglipron clinical program. The Phase 2b VISTA trial tracking pure obesity demonstrated a highly competitive profile, pushing out to a -11.8% weight reduction at 36 weeks without showing an immediate plateau. The parallel Phase 2b SOLSTICE trial underscored the molecule’s glycemic potency. Elecoglipron achieved a powerful -1.9% reduction in HbA1c at 26 weeks, enabling an impressive 90% of enrolled patients to reach the ADA’s target threshold of < 7.0%.
Two China-based biotechs discussed presented data for their oral GLP-1 agonists. Innovent turned heads with a striking Phase 1 multiple ascending dose readout. In a pure obesity cohort, IBI3032 triggered a rapid -10.11% body weight reduction in just 4 weeks. This double-digit drop in a single month suggests an exceptionally potent kinetic and bioavailable profile. Ascletis rounded out the oral landscape by presenting Phase 2 data for ASC30. In its obesity cohort, the asset demonstrated a steady, linear therapeutic trajectory, delivering a -7.7% weight loss at 13 weeks at the maximum dose tested.
Getting Up to Speed on Obesity?
Check out my two-part Frontiers in Medicine series here:
Obesity, Part 1

Societal perception, recognition as a disease, and the discovery of its hormonal & genetic drivers

To contact us, please send us an email at biotechreadout@gmail.com
Disclaimers
Investigational Status Disclaimer
The therapeutic candidates discussed in this newsletter are currently in clinical development and have not been approved for commercial sale by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), or other global regulatory authorities. Their safety and efficacy have not been established. References to pipeline products and ongoing clinical trials involve significant risks and uncertainties. Statements regarding the potential safety, potency, or efficacy of investigational drugs reflect current hypotheses and are not a guarantee of future performance or regulatory clearance. The outcome of clinical trials is inherently unpredictable, and clinical results from earlier stages may not be predictive of results in later, larger-scale trials.
No Medical Advice Disclaimer
This newsletter is for informational and educational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this publication.
No Patient-Provider Relationship Disclaimer
The information provided in this newsletter is for educational and analytical purposes only. Receipt of this information, or any interaction with this content, does not create a physician-patient, pharmacist-patient, or any other professional-provider relationship between you and the authors or publishers. This newsletter should not be used as a substitute for a personal consultation with a qualified healthcare professional.
Forward-Looking Statements Disclaimer
This newsletter contains “forward-looking statements” regarding future events, including clinical trial timing, regulatory milestones, and projected market performance. These statements are based on current expectations and assumptions that are subject to significant risks and uncertainties. Actual results may differ materially from those expressed or implied. We undertake no obligation to update these statements as a result of new information or future developments.
Third-Party Links & Content Disclaimer
This newsletter contains links to third-party websites, including clinical trial registries and corporate presentations. Biotech Readout does not endorse, guarantee, or assume responsibility for the accuracy or reliability of any information offered by third-party providers.
Errors and Omissions Disclaimer
While we strive for technical accuracy, the information in this newsletter is provided on an “as is” basis with no guarantees of completeness, accuracy, or timeliness. Biotech Readout assumes no liability for any errors or omissions in the content of this publication.
Non-Endorsement Disclaimer
Any reference to specific commercial products, processes, or services by trade name, trademark, or manufacturer does not constitute or imply an endorsement or recommendation by the author. All trademarks are the property of their respective owners.
No Investment Advice Disclaimer
This newsletter is for informational purposes only and does not constitute financial, investment, or legal advice. The author is not a registered investment advisor. You should consult with a professional financial advisor before making any investment decisions. The biotechnology sector is highly volatile; past performance is not indicative of future results.
Conflict of Interest Disclaimer
The author of this newsletter maintains a position of independence. At the time of publication, the author holds no direct financial interest, equity, or options in any of the companies mentioned in this report. No compensation has been received from any third party to feature or analyze specific therapeutic candidates or corporate entities.