
Eli Lilly to Acquire AtaiBeckley
SSRI/SNRI powerhouse bets on neuroplasticity for depression

Disclaimer: This newsletter is for educational and informational purposes only and does not constitute medical, investment, or financial advice, nor does it establish a provider-patient relationship. Content may include forward-looking statements and discussions of investigational therapeutic candidates that are not FDA/EMA approved; their safety and efficacy remain unestablished and clinical outcomes are unpredictable. While we strive for accuracy, all information is provided as is without guarantees. As of the date of publication, the author holds no direct equity positions in the specific companies mentioned in this issue nor receives third-party compensation for this coverage. Note that several of the compounds discussed, including psilocybin, DMT, and MDMA, are classified as Schedule I controlled substances under the U.S. Controlled Substances Act. Please find a complete version of our disclaimers linked here.

If you are a paid subscriber, go to this article’s premium charts & analysis here ⬇️
If you are a free reader or subscriber, enjoy the whole article free of charge and consider upgrading for premium charts & analysis on the depression landscape.
Introduction
On July 16, 2026, Eli Lilly and Company announced a definitive agreement to acquire AtaiBeckley for upfront cash consideration of approximately $2.8 billion plus up to approximately $1.0 billion Contingent Value Right (CVR), for a total deal value of up to $3.8 billion (Eli Lilly press release, AtaiBeckley press release). This acquisition centers on AtaiBeckley’s portfolio of investigational psychedelics for depression or anxiety:
BPL-003 (nasal 5-MeO-DMT): This their lead program and is being developed for treatment-resistant depression (TRD). It has been granted FDA Breakthrough Therapy Designation and is ready for Phase 3 clinical development.
VLS-01 (oral 5-MeO-DMT): This is a proprietary oral transmucosal film formulation of DMT. By utilizing a dissolving film (similar to a breath strip), it is designed to provide a more patient-friendly, in-clinic alternative to intravenous administration, with a targeted psychedelic effect duration of roughly 30-45 minutes. It is currently in Phase 2 clinical development.
ELE-101 (IV psilocin): This is a synthetic intravenous formulation of psilocin, the active metabolite of psilocybin. By administering the active compound directly, it is designed to offer more consistent dosing, a faster onset of action, and a shorter overall treatment duration (approximately two hours) compared to traditional oral psilocybin. It is currently in Phase 1/2a clinical development for major depressive disorder (MDD). A peer in the space, Compass Pathways, recently reported a positive Phase 3 trial for their formulation of synthetic psilocybin (COMP360) in TRD, which bodes well for this class.
EMP-01 (oral R-MDMA): This is an oral formulation of the R-enantiomer of MDMA, which is being investigated for the treatment of social anxiety disorder (SAD). Unlike traditional MDMA (which is typically a racemic mixture), EMP-01 is being studied for its potential therapeutic effects without requiring adjunctive psychotherapy. It has completed an exploratory Phase 2a trial, but it unfortunately missed its primary endpoint.
We will cover a more comprehensive history and landscape of depression medicines in a future Frontiers in Medicine piece. In this article, we briefly opine on the medical challenges of managing depression, dive into the story of AtaiBeckley, and explore how their neuroplastogen approach differs from traditional anti-depressants.
I should note that, as of the time of this publication, substances such as psilocybin, DMT, and MDMA remain classified as Schedule I controlled substances by the U.S. Drug Enforcement Agency (DEA). This classification underscores the significant regulatory framework that Eli Lilly/AtaiBeckley must navigate to move these investigational candidates through clinical development, as well as the ethical challenges that different people may have about this type of clinical research.
Reconnecting the Dots
The complexity of the human brain is often described as the most challenging frontier in modern science. With roughly 86 billion neurons and trillions of synaptic connections, the brain functions as a dynamic, non-linear network where structure and activity are in constant flux. When we attempt to map this complexity onto a condition like depression, we encounter a tension between our ability to observe the brain and our conceptual ability to understand it.
Most organs are defined by their specialized mechanical or chemical outputs. The heart is a pump. Its primary function (moving blood) remains consistent throughout life. The kidneys filter toxins based on blood pressure and osmolarity. While they react to environmental stressors, their functional goals (e.g., maintain fluid balance, clear waste) are fixed. The brain has no singular output in the traditional sense. It processes information, stores memory, generates consciousness, and regulates behavior. Crucially, it exhibits neuroplasticity: if a region of the brain is damaged, other regions can often be recruited to take over those functions. No other organ exhibits this degree of structural and functional re-allocation.
The complexity of the brain is further compounded by its vast connectivity. Organs like the stomach or pancreas function as distinct modules. They communicate with the rest of the body through hormones and the endocrine system, but their internal operation is largely self-contained. The brain is the only organ that must integrate inputs from every other system to function. It receives feedback from the endocrine system, the immune system, the gut microbiome, and the sensory organs, and integrates these into a unified internal map of the world. It is the only organ that is in communication with the entirety of the body simultaneously.
The brain’s ever-changing and highly interconnected nature makes neuroscience a study of emergent properties, rather than a study of discrete and well-defined bodily functions. Thoughts arise from the interplay of biochemical signaling (neurotransmitters), electrical activity (neuronal firing), and structural connectivity (white matter tracts). A change in one area, such as the prefrontal cortex, triggers a cascade of changes in distant regions like the amygdala or the hippocampus. It constantly rewires itself based on experience, environment, and internal chemistry. As a result of this plasticity, a snapshot of a depressed brain at one moment may look entirely different minutes or weeks later, making it difficult to establish fixed biomarkers.
The single factor that makes the study of depression challenging is this: there is no universal definition for what a depressed brain looks like. The biological underpinnings of depression in one person may be radically different from those in another, ranging from chronic systemic inflammation to genetic predisposition or dysregulated circadian rhythms. Although hard to measure through traditional medical technology, our lived experience tells us that depression is very much real.
Despite decades of research, our comprehension of the mechanisms causing depression remains incomplete, largely due to several systemic challenges. For many years, psychiatry operated under the monoamine hypothesis, the idea that depression was caused primarily by a deficiency of neurotransmitters like serotonin or norepinephrine. While effective treatments like selective serotonin reuptake inhibitors (SSRIs) and serotonin and norepinephrine reuptake inhibitors (SNRIs) target these systems, the medical community has come to recognize this view is overly reductionist. For the 1 in 3 people living with Major Depressive Disorder (MDD) who are failed by at least two conventional treatments, the standard of care offers little more than chemical maintenance. Raising serotonin levels helps many, but it does not fix the underlying circuit-level dysfunction for everyone, suggesting that serotonin is a downstream effect rather than the root cause.
Perhaps the most difficult aspect of studying depression is that the condition itself creates a biological feedback loop. Stress hormones (like cortisol) have neurotoxic effects on the hippocampus, the very region responsible for learning and emotional regulation. This means that if someone has been depressed for a long time, the physical architecture of their brain has been altered by the condition, making it incredibly difficult to isolate the cause from the effect.
In recent years, the field has shifted away from looking for broken chemicals to looking for broken circuits. We now understand that depression often involves abnormal communication between the Default Mode Network (DMN), which governs self-referential thought, and the brain’s executive control centers. However, we do not fully understand why these circuits become rigid or hyper-connected in the first place, or how to reliably reset them without global side effects. In this vein, a class of small-molecule drugs called neuroplastogens have recently emerged as a potential way to remodel these brain circuits.
Unlike traditional antidepressants (such as SSRIs) that are once-daily pills aimed at chemical rebalancing of the brain, neuroplastogens are characterized by their ability to induce profound brain-level changes quickly. The class is comprised of two prototypic buckets:
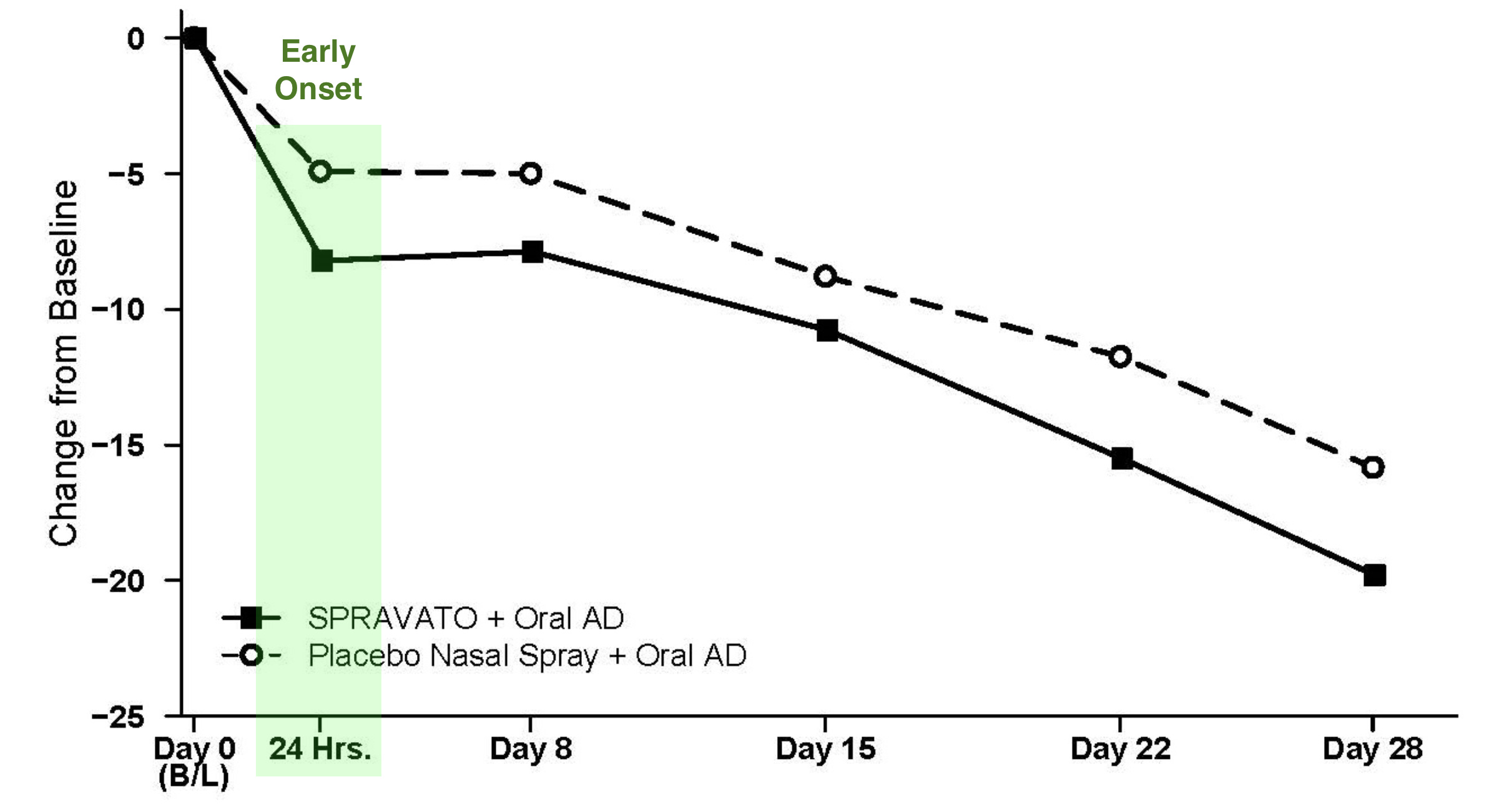
Ketamine-based: Spravato (esketamine) was the first ketamine-derived medication to receive FDA approval for Treatment-Resistant Depression (TRD) on March 5, 2019. Developed by Janssen (a Johnson & Johnson company), pivotal Phase 3 studies demonstrated that Spravato, when combined with an oral antidepressant, provided rapid and statistically significant improvements in Montgomery-Åsberg Depression Rating Scale (MADRS) scores compared to placebo plus an oral antidepressant. MADRS is an doctor-rated scale aimed at estimating the severity of depression. Benefits were frequently observed within 24 hours, providing a stark contrast to traditional antidepressants that often take several weeks to show effect.
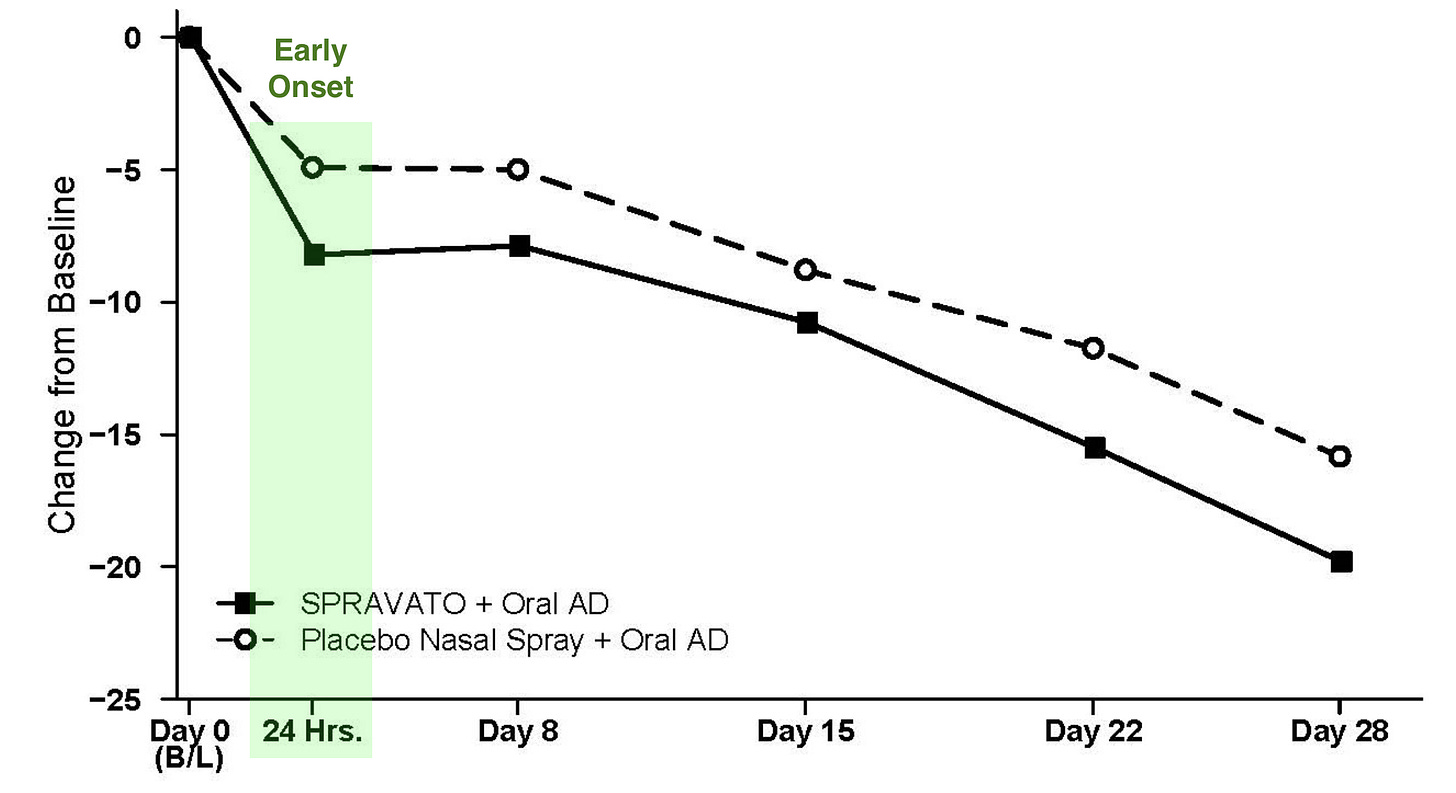
Least Squares Mean Change from Baseline in MADRS Total Score Over Time in Patients with TRD in Phase 3 TRANSFORM trial; Source: Spravato label, Table 5 Serotonergic Psychedelics: Compounds like psilocybin, DMT, 5-MeO-DMT, and LSD are potent neuroplastogens. They function through complex agonism of the 5-HT2A serotonin receptor and downstream activation of growth-signaling pathways like mTOR. As of the time of this publication, there are no FDA-approved serotonergic psychedelics for the treatment of depression, but this is the area that AtaiBeckley focused on.
Meeting of Minds
Meeting of Minds
AtaiBeckley is, in fact, a fusion of two companies that decided take on depression together. atai Life Sciences N.V. was founded in 2018 with the objective of developing medicines for mental health disorders, which the founders identified as a space suffering from a significant lack of innovation and high unmet medical need. The company was co-founded by three key individuals:
Christian Angermayer: A prominent investor and entrepreneur (founder of Apeiron Investment Group) who provided the foundational vision and early financial backing.
Florian Brand: Served as a key driver of the company’s operational and strategic growth, later becoming the CEO.
Lars Christian Wilde: Contributed specialized expertise to the company’s early development and platform strategy.
The founders were motivated by the disparity between the limited efficacy of existing psychiatric treatments and the growing global mental health crisis. They aimed to develop rapid-acting, durable, and convenient therapies for conditions like depression, anxiety, and addiction. Like others before them, they decided to utilize a hub-and-spoke model (centralize resources with modular programs), rather than operating as a traditional, monolithic pharmaceutical firm. atai was designed as a decentralized platform that incubates and supports subsidiary companies. This allowed the company to pool resources, regulatory expertise, and scientific best practices to accelerate the development of multiple assets simultaneously. From its origins as a startup based in Berlin, Germany, atai Life Sciences grew rapidly, securing significant capital from high-profile investors like Peter Thiel. The company eventually transitioned to a publicly traded entity, listing on the NASDAQ in June 2021. In late 2025, atai Life Sciences N.V. merged with Beckley Psytech Limited to form the current entity, AtaiBeckley Inc.
Beckley Psytech was founded in 2019 in Oxford, United Kingdom, as a for-profit clinical-stage biopharmaceutical company. The company was co-founded by a mother-son duo deeply embedded in the field of psychedelic research. Cosmo Feilding Mellen served as the company’s CEO and was the primary driving force behind its transition into a clinical-stage drug development firm. Lady Amanda Feilding was a globally recognized pioneer in psychedelic science who established the non-profit Beckley Foundation in 1998.
Beckley Psytech was built upon the decades of scientific research and advocacy work conducted by the Beckley Foundation. While the non-profit Foundation focused on scientific exploration and policy advocacy to reignite interest in psychedelic science, Beckley Psytech was established to take those scientific insights and translate them into licensed, regulated pharmaceutical medicines. The core mission of the company was to address the limitations of existing mental health treatments by developing rapid-acting, psychedelic-based therapies. Their research focus specifically prioritized compounds with a short time-in-clinic duration, aiming to create scalable treatments that could be safely administered and monitored in a healthcare setting, ideally with patient discharge possible within a few hours. Over its years as an independent private company, Beckley Psytech built a robust pipeline of novel psychedelic compounds, including their flagship asset BPL-003 (intranasal 5-MeO-DMT).
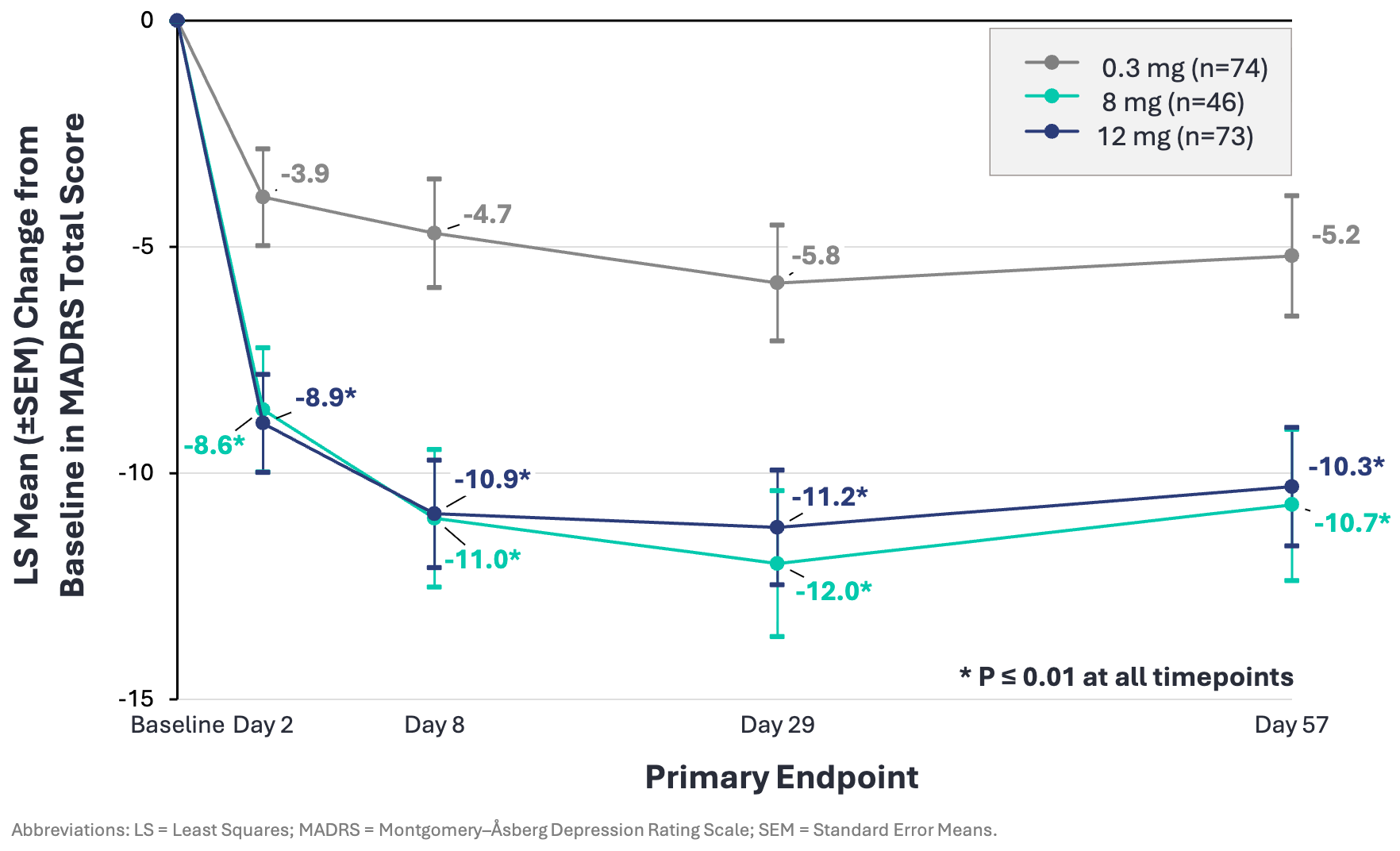
In July 2025, Beckley reported topline data for a Phase 2b study demonstrating that a single dose of BPL-003 produced statistically significant and durable reductions in depression scores (MADRS) in patients with Treatment-Resistant Depression (TRD). At Day 29, the 8mg dose showed a 12.1-point mean reduction in MADRS scores from baseline (vs. 5.8 in control). Statistically significant improvements were observed as early as Day 2 and were maintained through Week 8. This clinical success served as the catalyst for the merger and led to an FDA Breakthrough Therapy Designation. By mid-2026, the company had successfully aligned with the FDA on End-of-Phase 2 (EOP2) requirements, clearing the path for the initiation of Phase 3 trials. While the company’s current data is promising, it remains a hypothesis that these results will be replicated in larger, late-stage trials.
The evolution of AtaiBeckley culminated in its acquisition by Eli Lilly and Company, announced on July 16, 2026. The move signaled that a big pharma was willing to bet on the neuroplastogen thesis. Not just any big pharma, but an anti-depressant powerhouse that developed SSRI Prozac (fluoxetine) in the 1970s and SNRI Cymbalta in the early 2000s.
Conclusion
The acquisition of AtaiBeckley accelerates a shift in how the pharmaceutical industry approaches depression. By bringing BPL-003 and its neuroplasticity-focused pipeline into the fold, Eli Lilly evolves from the era of chronic chemical maintenance typified by Prozac and Cymbalta to an era of interventional, circuit-level repair. While the road to commercializing psychoplastogens remains fraught with clinical and regulatory hurdles, clinical & commercial successes like J&J’s Spravato suggests that the future lies in rewiring brain connections rather than rebalancing more brain chemicals.
Premium Charts & Analysis
All charts reflect data current as of the specified date and may not include every drug development program, although we aimed to capture the vast majority. Please feel free to email me at biotechreadout@gmail.com with “CHARTS” in the subject line to share suggestions or request chart updates.
Press ⬇️ to navigate to a section
