
Zymeworks to Acquire Theravance
M&A alchemy with a COPD sweetener

Disclaimer: This newsletter is for educational and informational purposes only and does not constitute medical, investment, or financial advice, nor does it establish a provider-patient relationship. Content may include forward-looking statements and discussions of investigational therapeutic candidates that are not FDA/EMA approved; their safety and efficacy remain unestablished and clinical outcomes are unpredictable. While we strive for accuracy, all information is provided as is without guarantees. As of the date of publication, the author holds no direct equity positions in the specific companies mentioned in this issue nor receives third-party compensation for this coverage. Please find a complete version of our disclaimers at the bottom of this article and on our About page.

Introduction
On June 29, 2026, Zymeworks Inc. announced a definitive agreement to acquire Theravance Biopharma, Inc. for approximately $929 million in cash consideration subject to customary adjustments (Zymeworks press release, Zymeworks slide deck, Theravance press release). This acquisition centers on Yupelri, a nebulized, once-daily, long-acting muscarinic antagonist (LAMA) for the maintenance treatment of chronic obstructive pulmonary disease (COPD).
In this article, we dive into the story of Yupelri’s development, identify its place in the COPD landscape, and discuss the deal’s unique business development angle.
Breathing Room
Chronic Obstructive Pulmonary Disease (COPD) is a progressive, inflammatory lung condition that causes long-term breathing difficulties by restricting airflow into and out of the lungs. Primarily caused by smoking or long-term exposure to airborne irritants, it encompasses chronic bronchitis (inflammation and mucus buildup in the bronchial tubes) and emphysema (the destruction of the lung’s fragile air sacs). Over time, this damage leads to persistent symptoms like shortness of breath, a chronic cough, and wheezing, which gradually worsen but can be managed with bronchodilators, lifestyle changes, and targeted anti-inflammatory therapies.
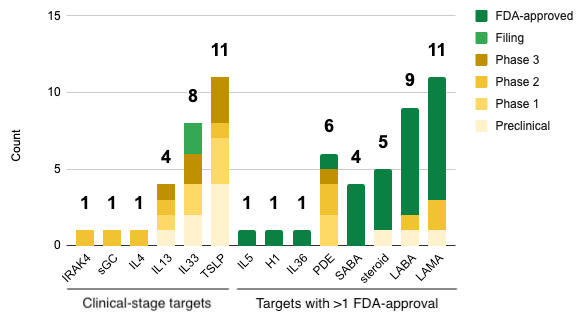
Yupelri represents an effort to deliver a long-acting bronchiodilator directly to the lungs, with the goal of relax airway smooth muscle and improve airflow in patients with COPD. Muscarinic antagonists are a relatively old drug class in the COPD space. Boehringer Ingelheim’s Atrovent (ipratropium bromide) achieved first-in-class status with its FDA approval on December 29, 1986. However, it was a short-acting muscarinic antagonist (SAMA), requiring patients to use it 3 to 4 times a day due to its short half-life. The early 2000s oversaw a race for long-acting muscarinic antagonists (LAMAs), which could provide similar relief as SAMAs but with the convenience of once daily dosing. Boehringer Ingelheim once again stood at the vanguard, securing the first LAMA approval for COPD with Spiriva HandiHaler (tiotropium bromide) on January 30, 2004. Today, LAMAs are the drug class with the most FDA approvals in COPD (see graph below).
So, where did Yupelri come in? The active pharmaceutical ingredient in Yupelri is called revefenacin (initially designated as TD-4208) and was discovered by Theravance in the early 2000s. With their new medicine, Theravance set out to raise the bar for the COPD treatment landscape in two ways:
Enhance inhaled delivery using a nebulizer: While several long-acting LAMAs existed for handheld dry-powder or metered-dose inhalers, patients with severe or advanced COPD often lacked the inspiratory flow rate necessary to use those devices effectively. Theravance specifically developed TD-4208 as an inhalation solution designed to be compatible with standard jet nebulizers.
Make it safer by reducing systemic exposure: They applied their lung-selective chemistry platform to create a LAMA that was designed to provide sustained bronchodilation locally in the lungs while rapidly breaking down if it entered systemic circulation. This could minimize classic anticholinergic side effects, such as dry mouth and urinary retention, that frequently occur with systemic exposure.
In 2015, Theravance entered into a strategic collaboration with Mylan to advance the asset through late-stage global clinical trials and commercialization. Under the agreement, Theravance led the U.S. clinical development program, while Mylan heavily financed the registrational path and managed ex-U.S. expansion. Theravance retained a U.S. profit-sharing model and global rights to alternative delivery formats (like MDI/DPI inhalers).
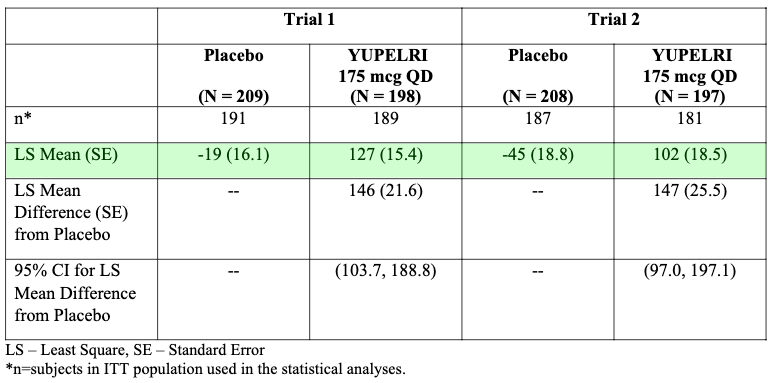
The clinical path to approval culminated in an extensive Phase 3 program evaluating more than 2,300 patients with moderate-to-very-severe COPD. Two identical 12-week pivotal Phase 3 efficacy trials demonstrated that a once-daily dose of revefenacin led to statistically significant and clinically meaningful improvements in trough forced expiratory volume in one second (FEV1) compared to placebo (+102-127 mL for Yupelri versus -19-45 for placebo; see table below). In July 2017, Theravance and Mylan announced positive results from a large, 1,055-patient, 12-month Phase 3 safety study. The data showed that revefenacin was well-tolerated over long periods, whether used as a standalone maintenance bronchodilator or as an add-on to other COPD regimens, such as LABAs or ICS/LABA combinations.
Backed by successful Phase 3 efficacy and safety data, Yupelri’s New Drug Application (NDA) was filed in late 2017. On November 9, 2018, the U.S. Food and Drug Administration officially granted market authorization for Yupelri (revefenacin) inhalation solution for the maintenance treatment of patients with COPD. In June 2019, Theravance and Mylan expanded their collaboration agreement to grant Mylan exclusive development and commercialization rights for nebulized revefenacin in China and adjacent territories, tapping into an underserved market of nearly 100 million COPD patients. In late 2020, Mylan merged with Pfizer’s off-patent medicine division (Upjohn) to form Viatris. Consequently, commercial marketing and co-promotion responsibilities for Yupelri transitioned under the Viatris banner.
While the success of Yupelri created breathing room for Theravance, the rest of their pipeline was defined by a sequence of high-profile clinical trial stumbles. Ampreloxetine, a once-daily selective norepinephrine reuptake inhibitor (NRI), was Theravance’s flagship late-stage asset behind Yupelri. It was designed to treat neurogenic orthostatic hypotension (nOH), a severe drop in blood pressure upon standing, in patients with rare neurodegenerative conditions. However, it failed three separate Phase 3 trials (Study 0169 in 2021, REDWOOD in 2022, CYPRESS in 2026) and ultimately landed on the out-licensing list. Nezulcitinib (TD-0903) was an inhaled, lung-selective Janus kinase (JAK) inhibitor being developed to treat acute lung injury, chronic lung inflammation, and fibrotic lung diseases (including severe COVID-19-associated lung injury). It was discontinued after a Phase 2 trial reported in 2023 failed to show clinical efficacy. Before focusing exclusively on ampreloxetine and respiratory medicine, Theravance attempted to develop an oral, gut-selective JAK inhibitor for inflammatory bowel disease (IBD) in collaboration with Janssen (Johnson & Johnson). That too met an untimely end when, in late 2021, it missed its primary endpoint of clinical remission in a Phase 2b/3 trial for ulcerative colitis.
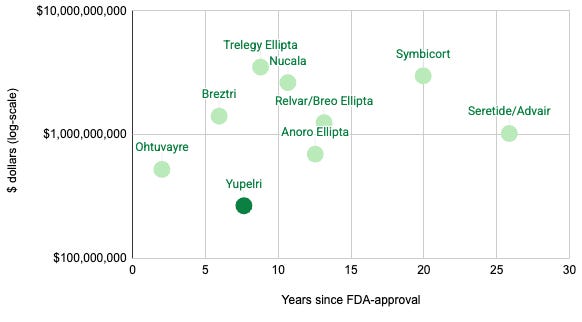
In June 2026, oncology and immunology biopharma company Zymeworks announced a definitive agreement to acquire Theravance Biopharma for roughly $929 million. The acquisition explicitly absorbed Theravance’s remaining financial stakes in Yupelri. While Yupelri generated an impressive $266.6 million in U.S. net sales in 2025, it has been overtaken by dual or triple single-inhaler therapies that combine muscarinic agonists, beta agonists, and corticosteroids (Trelegy Ellipta, Breztri, and others) and novel mechanisms (such as the anti-IL5 mAb Nucala for eosinophilic phenotypes of COPD).
Acquisition Alchemy
To be clear, the Biotech Readout is not a financial newsletter. However, Zymeworks’ deal structure is creative enough to merit a brief discussion.

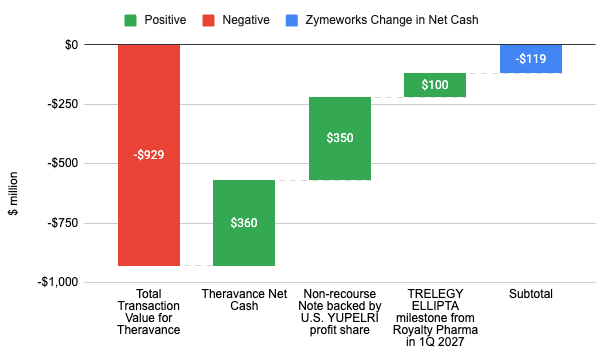
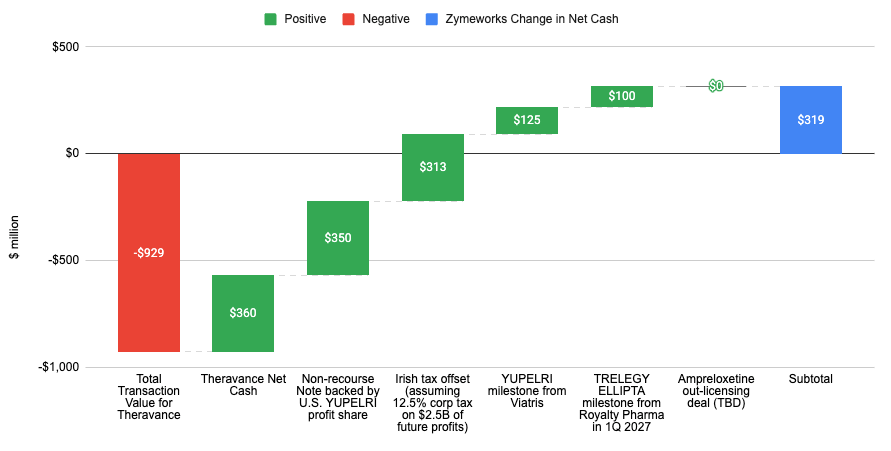
While the total cash consideration of acquiring Theravance is approximately $929 million, Zymeworks only expects to pay out $119 million in net cash at close (see graph below). How is it that they only need to pay out about 1/8 of the total deal value? Theravance’s net cash on the balance sheet, a non-recourse note backed by U.S. YUPELRI profit share, and a milestone from Royalty Pharma for Trelegy Ellipta expected in 1Q 2027 reduce Zymeworks’ net cash requirements by a combined $810 million. That’s not even the half of it.
When accounting for other milestones and tax offsets mentioned in their press release, Zymeworks could actually gain $319 million in net cash from the acquisition (see graph below) leaving them with Yupelri, an asset pro-forma modeled to generate an estimated $15 million per year (derived from the ~$60 million annualized cash flow mentioned in the press release minus the 75% profit share owed to OMERS Life Sciences). Yes, there is a scenario where Zymeworks could actually make money by acquiring another company. Out-licensing the investigational asset ampreloxetine could add additional cash to Zymeworks’ haul.
Clever investment bankers indeed.
Conclusion
The saga of Theravance and Yupelri highlights the unpredictable nature of drug development. Pipeline stumbles can dismantle even the most veteran R&D organizations, but a single well-designed, organ-selective molecule can establish a permanent footprint within the standard of care. As for Zymeworks, their acquisition of Theravance is a masterclass in creative deal structures. While Yupelri never quite transformed into the commercial blockbuster its early developers envisioned, its durable cash flows in a highly resilient niche provided Theravance with an exit. By structuring a transaction that mitigates capital risk, Zymeworks has secured a steady commercial baseline while preserving its firepower for downstream oncology innovation.
Love biotech? Check out Biotech Readout’s full content library, or navigate directly to a segment that interests you:
Frontiers in Medicine: Exploring the frontiers of our understanding and treatments for disease.
Medical History: Recovering forgotten relics in the history of medicine.
Acquisitions: Exploring the innovation behind acquired companies.
Weekly Readout: A digest of new clinical data from the past week.
To contact us, please send us an email at biotechreadout@gmail.com
Disclaimers
Investigational Status Disclaimer
The therapeutic candidates discussed in this newsletter are currently in clinical development and have not been approved for commercial sale by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), or other global regulatory authorities. Their safety and efficacy have not been established. References to pipeline products and ongoing clinical trials involve significant risks and uncertainties. Statements regarding the potential safety, potency, or efficacy of investigational drugs reflect current hypotheses and are not a guarantee of future performance or regulatory clearance. The outcome of clinical trials is inherently unpredictable, and clinical results from earlier stages may not be predictive of results in later, larger-scale trials.
No Medical Advice Disclaimer
This newsletter is for informational and educational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this publication.
No Patient-Provider Relationship Disclaimer
The information provided in this newsletter is for educational and analytical purposes only. Receipt of this information, or any interaction with this content, does not create a physician-patient, pharmacist-patient, or any other professional-provider relationship between you and the authors or publishers. This newsletter should not be used as a substitute for a personal consultation with a qualified healthcare professional.
Forward-Looking Statements Disclaimer
This newsletter contains “forward-looking statements” regarding future events, including clinical trial timing, regulatory milestones, and projected market performance. These statements are based on current expectations and assumptions that are subject to significant risks and uncertainties. Actual results may differ materially from those expressed or implied. We undertake no obligation to update these statements as a result of new information or future developments.
Third-Party Links & Content Disclaimer
This newsletter contains links to third-party websites, including clinical trial registries and corporate presentations. Biotech Readout does not endorse, guarantee, or assume responsibility for the accuracy or reliability of any information offered by third-party providers.
Errors and Omissions Disclaimer
While we strive for technical accuracy, the information in this newsletter is provided on an “as is” basis with no guarantees of completeness, accuracy, or timeliness. Biotech Readout assumes no liability for any errors or omissions in the content of this publication.
Non-Endorsement Disclaimer
Any reference to specific commercial products, processes, or services by trade name, trademark, or manufacturer does not constitute or imply an endorsement or recommendation by the author. All trademarks are the property of their respective owners.
No Investment Advice Disclaimer
This newsletter is for informational purposes only and does not constitute financial, investment, or legal advice. The author is not a registered investment advisor. You should consult with a professional financial advisor before making any investment decisions. The biotechnology sector is highly volatile; past performance is not indicative of future results.
Conflict of Interest Disclaimer
The author of this newsletter maintains a position of independence. At the time of publication, the author holds no direct financial interest, equity, or options in any of the companies mentioned in this report. No compensation has been received from any third party to feature or analyze specific therapeutic candidates or corporate entities.