
Listerine to Lipitor
A 173-year pharmaceutical odyssey of Warner-Lambert

Disclaimer: This newsletter is for educational and informational purposes only and does not constitute medical, investment, or financial advice, nor does it establish a provider-patient relationship. Content may include forward-looking statements and discussions of investigational therapeutic candidates that are not FDA/EMA approved; their safety and efficacy remain unestablished and clinical outcomes are unpredictable. While we strive for accuracy, all information is provided as is without guarantees. This newsletter is independent, and the author holds no financial positions in the companies mentioned nor receives third-party compensation for this coverage. Please find a complete version of our disclaimers at the bottom of this article and on our About page.

Introduction
To the modern observer, Warner-Lambert is an often-forgotten ghost of corporate eras past; a name buried beneath decades of rapid consolidation, mega-mergers, and shifting corporate rebrandings. Yet, just a generation ago, this titan stood as a heavyweight of the pharmaceutical industry, commanding a sprawling, multi-billion-dollar empire that straddled medicines and everyday consumer goods.
Crucially, the foundation of this empire was forged during one of the greatest paradigm shifts in human history from the miasma theory to the germ theory of disease. The company’s earliest corporate ancestors commercialized this paradigm shift, creating one of history’s most iconic brands, Listerine. It was a spectacular R&D bet more than a hundred years later in their cardiovascular pipeline that would ultimately define their legacy and seal their corporate fate. As latecomers to a fiercely competitive class of medications, Warner-Lambert’s research engine defied the odds to develop Lipitor (atorvastatin), a synthetic molecule that exploded into the best-selling prescription drug in medical history (although it has since been surpassed).
Here, we dive into the remarkable story of Warner-Lambert, a 173-year pharmaceutical odyssey from Listerine to Lipitor.
The Makings of a Surgeon
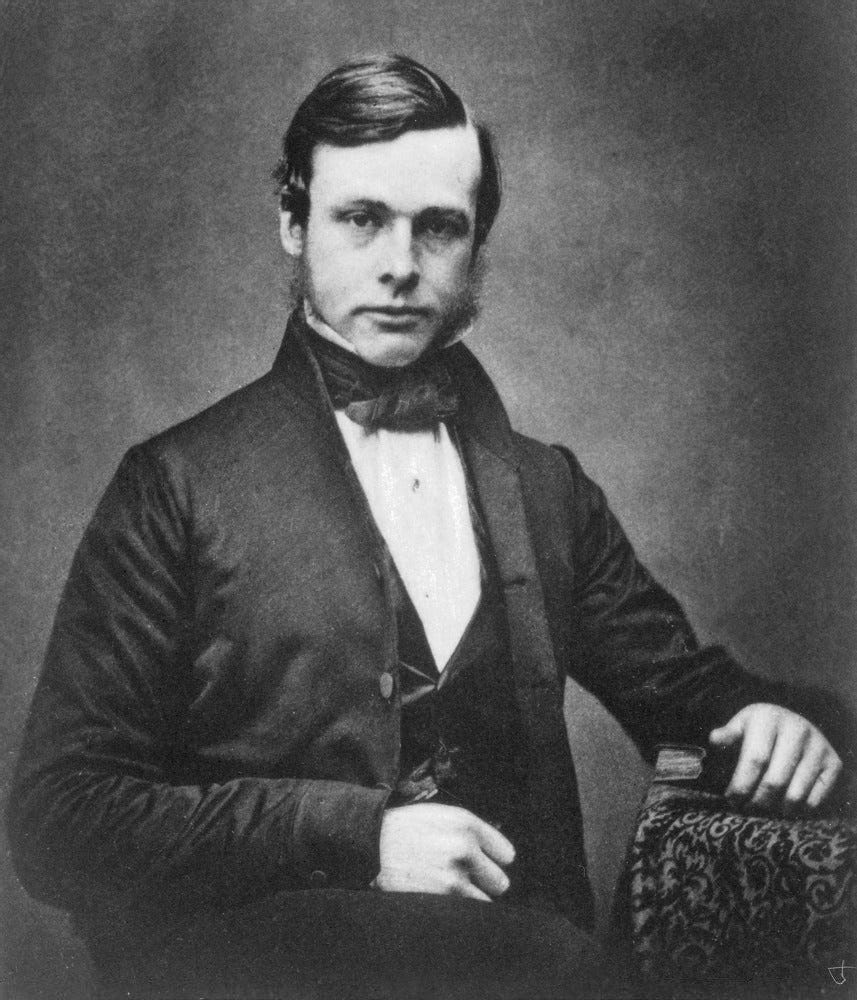
Joseph Lister was born in 1827 into a prosperous, devout Quaker family in the village of Upton in England. His father, Joseph Jackson Lister, was a wine merchant by trade but a scientist at heart. Frustrated by the blurred, distorted images produced by early microscopes, the elder Lister spent his evenings working through optical mathematics. He eventually invented the achromatic lens, a breakthrough that eliminated the rainbow-like distortion of light and laid the foundation for modern microscopy. Under his father’s gentle guidance, young Joseph spent his childhood looking past the surface of things. He dissected birds and small mammals, mapping their tissues under the family’s state-of-the-art lenses. By the time he was a teenager, he knew two things with absolute certainty: he wanted to understand the living architecture of the human body, and he wanted to be a surgeon.
In 1844, at seventeen, Lister entered University College London (UCL). As a Quaker, he was barred from attending Oxford or Cambridge, which required swearing oaths to the Church of England. UCL, known as the “Godless College” for its radical inclusivity, proved to be the perfect crucible for a young scientist. He returned to London with a hardened resolve. In 1850, he witnessed a key innovation in medicine: the first operations using ether at University College Hospital. Surgery was suddenly painless, but it was not yet safe. Lister watched in frustration as patients sailed through painless amputations, only to rot from mysterious wound infections days later. He graduated with his medical degree in 1852.
Seeking to refine his surgical hands, Lister traveled to Edinburgh in 1853 to study under Professor James Syme, widely regarded as the greatest clinical surgeon of the generation. Syme was a master of speed and precision, but more importantly, he became Lister’s mentor, advocate, and surrogate father. Lister’s meticulous nature quickly won Syme over. Within a few years, Lister was appointed as Syme’s first assistant. He also fell in love with Syme’s daughter, Agnes. To marry her, Lister made the agonizing decision to leave the Quaker faith, as marrying outside the Society was strictly forbidden. They wed in 1856.
{kind=link}
Agnes was much more than a housewife to Lister. She was an intellectual partner. Fluent in French and German, she possessed a sharp scientific mind. Throughout their marriage, she spent her nights sitting across from Lister in their home laboratory, writing down his dictated observations, translating foreign scientific papers, and cleaning his microscopes. Together, they began researching inflammation. Using his father’s achromatic lenses, Lister peered at the capillaries of frogs and bats, trying to understand how blood vessels responded to injuries. He grew convinced that wound rot wasn’t a failure of the blood, but an active, aggressive process triggered by something external.
The culmination of Lister’s long preparation arrived in 1860, when he was appointed Regius Professor of Surgery at the University of Glasgow. At thirty-three, he was entering the prime of his career, responsible for the bustling wards of the Glasgow Royal Infirmary. The infirmary was a massive, overcrowded facility catering to the victims of Glasgow’s heavy industrial factories and shipyards. Compound fractures, where shattered bones tore through the skin, flooded his ward. Lister washed his hands, kept his ward as clean as the prevailing standards dictated, and yet, the results were horrifying. Nearly half of his amputation cases ended in the same grisly manner: localized inflammation, a sickly sweet odor, blackening flesh, a spiking fever, and death. The medical establishment blamed “miasma”, foul spontaneous gases thought to be generated by the crowded hospital itself. However, Lister’s lifelong training with the microscope made him deeply skeptical. He noticed that if a bone broke cleanly inside the leg, the patient healed. If the skin tore open to the air, the leg rotted.
Sitting in his study in Glasgow, surrounded by pages of notes taken in Agnes’s neat handwriting, Lister looked at the data. It wasn’t the bone, and it wasn’t the blood. The air was introducing a ghost into the wound. Armed with his father’s lessons on optics and his own decade of surgical observation, Lister stood on the precipice of his life’s great work. He just needed a catalyst to show him exactly what the air was carrying.
Born to Fight Miasmas, Forced to Fight Germs
Derived from the ancient Greek word for “pollution” or “stain,” miasma theory contended that diseases like cholera, malaria, and the Black Plague were caused by inhaling “bad air”, a noxious and foul-smelling vapor filled with decaying organic matter. It dictated that diseases were not passed from person to person. Instead, they were localized environmental hazards born from filth, rotting vegetation, swamps, and stagnant water.
{kind=link}
To a pre-microscope world, miasma theory made intuitive sense because it aligned with human senses: where there was disease, there was almost always a terrible smell. According to physicians of the era, breathing in these toxic mists corrupted the body’s internal balance. The theory operated on a few core assumptions:
The Scent of Death: If a neighborhood smelled like open sewage, rotting garbage, or swamp gas, a miasma was present, and an outbreak was imminent.
Environmental Triggers: Changes in the weather, low-lying geographic areas (like valleys and marshes), and poor ventilation trapped miasmas close to the ground.
Spontaneous Generation: Wounds didn’t get infected because something entered them; rather, the ambient miasma in a hospital caused the exposed flesh to spontaneously rot and decay.
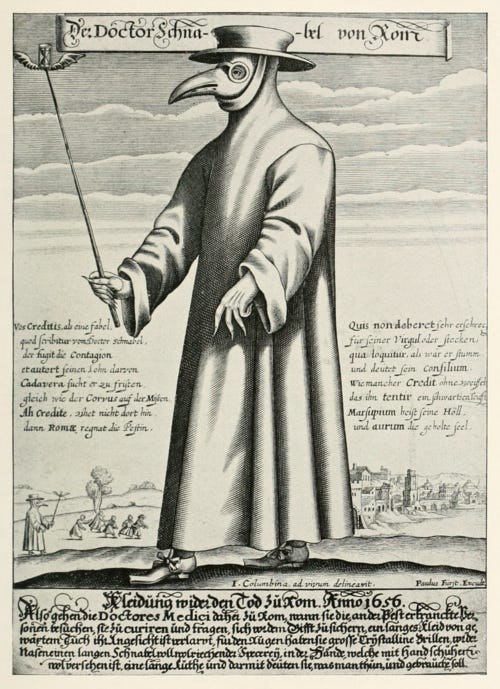
Since people believed the air itself was the enemy, centuries of public health, urban planning, and architecture were designed specifically to fight bad smells and stagnant air. The iconic bird-like masks worn by 17th-century plague doctors were not meant to look scary. The long beaks were packed with aromatic spices, dried flowers (like roses or carnations), camphor, and mint. The goal was to filter out the deadly miasma with pleasant scents. Victorian hospitals were built with massive windows, soaring ceilings, and cross-ventilation corridors (known as the “Nightingale style”). The goal was to constantly flush out the corrupted indoor air.
.png){kind=link}
Miasma theory had been the prevailing medical theory of disease ever since it originated with Hippocrates in the fifth century BC. That dogma changed when, in the summer of 1856, a distressed local businessman walked into the chemistry laboratory at the University of Lille, desperate for help. He was an industrial distiller who made alcohol from beetroot juice, but his vats were failing. Instead of producing clean, profitable alcohol, his beetroot soup was turning into a slimy, sour, foul-smelling mess. The man he came to see was thirty-three-year-old Louis Pasteur.

{kind=link}
At the time, Pasteur was not a physician or a biologist; he was a brilliant young chemist famous for his work on crystal symmetry. The scientific consensus of the day dictated that fermentation (the process that turns sugar into alcohol) was a purely chemical, dead reaction. If wine or beetroot juice went sour, it was believed to be a spontaneous chemical malfunction. Pasteur, armed with a microscope and an insatiable curiosity, agreed to visit the distillery. He collected samples from both the healthy, bubbling vats and the sick, slimy ones, and returned to his laboratory to look closer.
Under his microscope, Pasteur noticed a stark biological contrast:
In the healthy vats where alcohol was forming, the liquid was filled with tiny, plump, golden-round globules. These were yeast cells, living organisms.
In the sour vats, the round cells were entirely absent. Instead, the liquid swarmed with millions of tiny, elongated rod-like structures.
Pasteur had a profound realization: fermentation was the product of microscopic organisms, not a purely chemical reaction. The round yeast cells were eating the sugar and producing alcohol. But when the rod-shaped organisms invaded, they overran the yeast, ate the sugar, and excreted lactic acid, ruining the batch. This discovery laid the groundwork for what would become pasteurization, the process of heating liquids just enough to kill the invasive, unwanted microbes without altering the flavor of the product. But for Pasteur, it triggered an even greater, world-altering hypothesis: If microscopic invaders could make a vat of beetroot juice physically sick, could they do the same thing to a human being?
Before Pasteur could convince the scientific world that invisible organisms caused human illness, he had to destroy a deeply entrenched myth: Spontaneous Generation. As mentioned before, this aspect of miasma theory contended that life routinely sprang from non-living matter. It was mistakenly believed that maggots spontaneously generated out of rotting meat and mice grew out of damp piles of straw.
To prove his theory that microscopic organisms were responsible for fermentation, Pasteur designed one of the most elegant, famous experiments in scientific history: the swan-neck flask experiment. Pasteur poured nutrient-rich meat broth into glass flasks. He then heated the glass necks of the flasks, melting and bending them into long, elegant S-curves, resembling the neck of a swan.
Sterilization: He boiled the broth inside the flasks to kill any existing microbes.
Filter: Air could freely flow in and out of the curved opening, but any airborne dust, mold, or bacteria would get trapped by gravity in the bottom curve of the long, narrow neck.
Result: The broth remained perfectly clear and sterile for months. Life did not spontaneously appear.
Reversal: When Pasteur finally tilted a flask so that the pristine broth washed into the dusty, curved neck and ran back down, the broth became cloudy and swarmed with microbes within 48 hours.
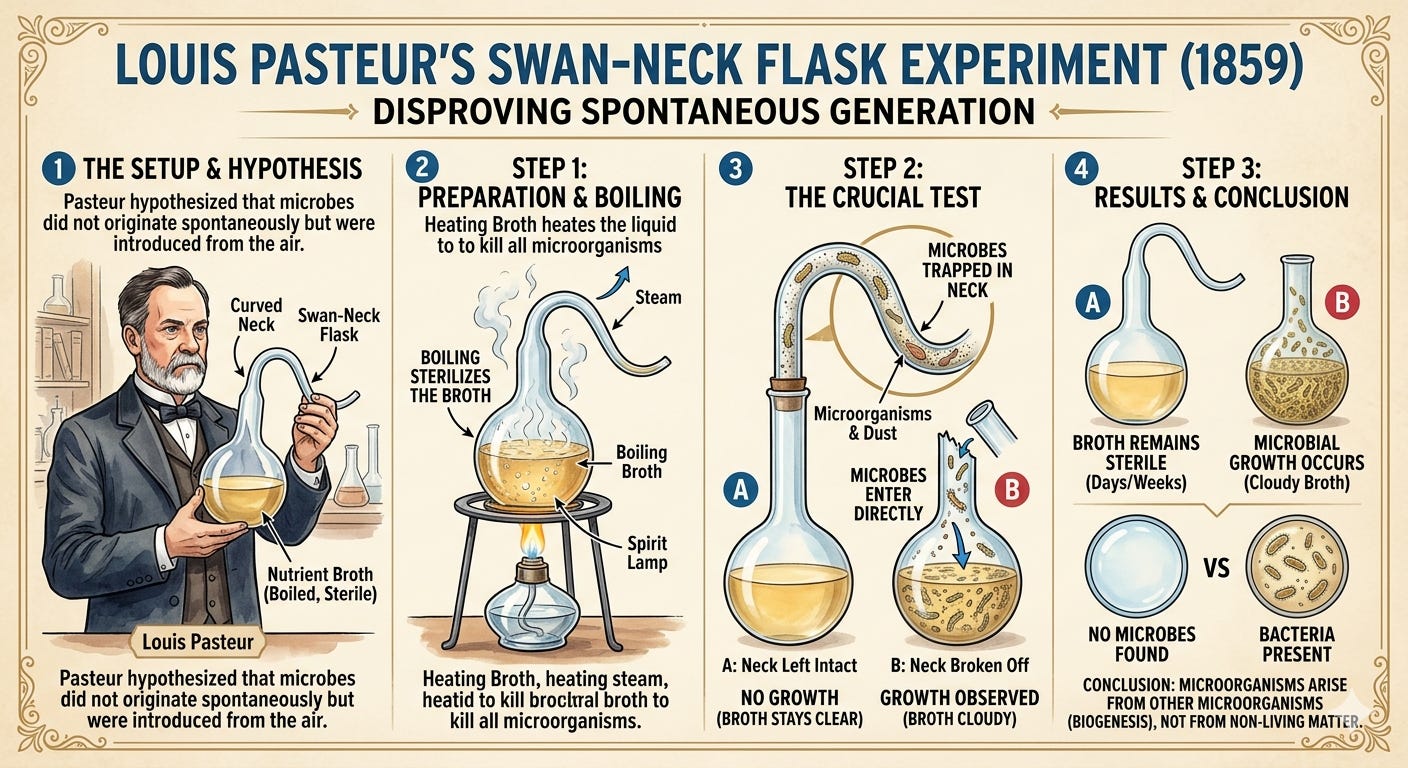
Pasteur had demonstrated definitively that decay, rot, and microbial life came from the outside world. The air was a transport system for living organisms. By the late 1860s, Pasteur’s attention shifted fully from industrial chemistry to human medicine. He was driven in part by immense personal tragedy: he lost three of his five children to typhoid fever, a brutal reminder of humanity’s helplessness against infectious disease. Pasteur began applying his germ theory of disease to various outbreaks, systematically proving that specific microscopic pathogens were linked to specific illnesses:
The Silkworm Crisis (1865): Pasteur saved the French silk industry by isolating a microscopic parasite attacking silkworms and their eggs, proving that a living microbe could cause an epidemic.
Chicken Cholera & Immunization (1879): Accidentally discovered that old, weakened cultures of chicken cholera bacteria didn’t kill the birds, but instead immunized them against future, lethal doses. In doing so, Pasteur discovered the principle of artificial vaccines.
The Anthrax Demonstration (1881): In a dramatic public experiment at a farm in Pouilly-le-Fort, Pasteur successfully vaccinated sheep against deadly anthrax, cementing the germ theory in the public consciousness.
The Rabies Vaccine (1885): Pasteur faced his ultimate test when nine-year-old Joseph Meister was savaged by a rabid dog. Pasteur treated the boy with a series of weakened rabies nerve-tissue injections. The boy survived, marking a monumental triumph for human medicine.
This brings us back to Joseph Lister’s puzzling dilemma: nearly half of his amputation cases ended in localized inflammation, blackening flesh, spiking fevers, and death. Were miasmas infiltrating the tissue, or was there another explanation?
The missing piece of the puzzle arrived in the form of a recommendation from a colleague, Thomas Anderson, a professor of chemistry at Glasgow. Anderson handed Lister a French research paper published by Louis Pasteur. As Lister read Pasteur’s work, the clouds of the miasma theory evaporated. Pasteur’s research demonstrated that microscopic, living organisms (“germs”) carried through the air were the true culprits behind fermentation and putrefaction. Lister realized that human flesh was no different than milk or wine. Wounds didn’t rot because of the air itself; they rotted because the air was a highway for invisible, living invaders. To save his patients, Lister needed a chemical barrier to kill the microbes before they could breach the flesh.
In 1865, Lister turned to a crude, dark fluid called carbolic acid, which he knew had been used to safely neutralize the odor and parasites in municipal sewage. He formulated a solution and waited for the right patient. On August 12, 1865, eleven-year-old James Greenlees was brought to the infirmary, his leg broken and bone protruding through a bloody tear in his skin. Instead of amputating the limb, Lister thoroughly cleaned the wound and applied a piece of lint soaked in carbolic acid, sealing it. Over the next several days, the boy experienced no fever, no pain, and none of the sickeningly sweet smell of gangrene. The wound remained clean and healed perfectly.
Lister spent the next two years meticulously refining his protocol. He treated eleven more compound fracture cases using carbolic acid dressings. Nine recovered completely, one required an amputation but survived, and only one died due to an unrelated internal hemorrhage. In a ward where a compound fracture was previously a near-certain death sentence, this improvement in survival was unprecedented.
Lister quickly realized that the entire operating environment was a source of contamination. In the 1860s, surgeons prided themselves on wearing stiff, blood-stained frock coats that were never washed, viewing the dried gore as a badge of experience. Surgical instruments were casually wiped on old rags or pants legs between operations, and hands were rarely washed. Lister began systematically dismantling these traditions, moving from simple wound treatment into a comprehensive system of antiseptic surgery:
Instrument Sterilization: Every scalpel, saw, and needle was soaked in a five percent solution of carbolic acid before touching a patient.
Hand Hygiene: Surgeons and assistants were forced to thoroughly wash their hands in carbolic solutions prior to incisions.
Catgut Sutures: Realizing that traditional silk threads left inside the body became breeding grounds for bacteria, Lister invented absorbable catgut sutures sterilized in carbolic oil.
To neutralize airborne germs in the operating theater itself, Lister developed a specialized mechanical device: a brass steam atomizer that he used to create a sterile zone around the operating table. The device pumped out a continuous, fine mist of carbolic acid over the operating table, coating the surgical site, the instruments, and the doctors. While the caustic spray made the surgeons’ fingers numb and irritated their lungs, it successfully created an unprecedented zone of safety for the patient.
In 1867, Lister published his astonishing findings in a series of papers in Lancet. While young doctors and continental European surgeons, particularly in Germany, embraced “Listerism” with enthusiasm, the older British and American medical establishments fiercely resisted. Prominent surgeons mocked the “germ theory,” complaining that the carbolic mist was messy, expensive, and unnecessary. Undeterred, Lister continued to accumulate data. He took his methods to Edinburgh and eventually to King’s College London in 1877, where he performed a highly publicized, daring operation to wire a fractured patella (kneecap), a procedure that would have been universally fatal under old methods. He performed it flawlessly under a cloud of carbolic mist, and the patient made a complete recovery.
Acceptance by the medical community accelerated in September 1879 at the Sixth International Medical Congress in Amsterdam, a global forum for medicine drawing hundreds of the world’s leading physicians, pathologists, and surgeons. Lister arrived not knowing quite how he would be received. When he stepped onto the stage of the grand lecture hall to deliver his address on the antiseptic system, the reaction was immediate and overwhelming. The entire assembly of international doctors rose to their feet. The hall erupted into a thunderous, rhythmic chanting of his name, accompanied by waving handkerchiefs and stomping feet. The applause lasted for several unbroken minutes. European doctors, many from nations like Germany and France that had recently been bitter battlefield enemies in the Franco-Prussian War stood shoulder-to-shoulder to honor a man whose innovations had saved thousands of wounded soldiers on both sides of the conflict. The spectacle at Amsterdam was a crushing blow to Lister’s remaining critics back home in England. It demonstrated that while London’s senior elite were still bickering over the existence of invisible germs, the rest of the civilized world had already moved forward, embracing Lister as a trailblazer.
Sixteen years after his triumph in Amsterdam, Lister achieved the ultimate recognition of his scientific brilliance. In 1895, he was elected President of the Royal Society, succeeding the iconic physicist Lord Kelvin. Founded in 1660, the Royal Society was the oldest and most prestigious scientific academy in continuous existence. To be elected its president was to be named the official leader of the British scientific empire, a position previously held by giants like Sir Isaac Newton and Sir Humphry Davy.
By the time Lord Lister passed away in 1912, the terrifying specter of “hospital gangrene” had been conquered. His relentless pursuit of cleanliness, rooted in an understanding of the microscopic world, converted the surgical theater from a chamber of post-operative doom into a modern sanctuary of healing.
Listerine of Lambert Pharmacal
The sharp, medicinal fog of carbolic acid that blanketed Joseph Lister’s Glasgow operating theater ignited a spark of inspiration that leaped across the Atlantic Ocean. While Lister was locked in a bitter struggle to convince the conservative medical elite of London that invisible germs were harbingers of a deadly scourge, a new breed of American entrepreneurs was watching his work with rapt attention, eager to democratize his radical philosophy of cleanliness.
The translation of Lister’s sterile technique from a surgical protocol into a commercial product found its epicenter in the bustling post-Civil War river port of St. Louis, Missouri. In the late 1870s, the concepts of germ theory and antiseptic care were still bleeding-edge science. To the average American, surgery remained a terrifying gamble, and everyday hygiene was rudimentary at best. Yet, two men saw a brilliant opportunity in Lister’s discoveries.
Ironically, they started with a profound flaw in Lister’s methodology: while carbolic acid was an effective germ-killer, it was highly caustic, notoriously burning the skin of surgeons and corroding human tissue. They asked a transformative question: Could they create a mild, non-toxic antiseptic that embodied Lister’s germ-destroying principles, but was safe enough for everyday medicinal use?
The story began in St. Louis, Missouri, in the late 1870s. Jordan Wheat Lambert, a charismatic twenty-something former clerk and insurance worker, was working for a local wholesale drug house. Lambert possessed a keen mind for commercial opportunities and was deeply fascinated by the revolutionary antiseptic surgical breakthroughs of Sir Joseph Lister in Great Britain. Through the tight-knit St. Louis medical and pharmaceutical scene, Lambert connected with Dr. Joseph Lawrence, a local physician and the editor of a prominent medical journal. Lawrence shared Lambert’s obsession with the new “germ theory” popularized by Louis Pasteur and Joseph Lister. In 1879, Dr. Lawrence successfully compounded a proprietary blend of volatile oils including eucalyptol, thymol, menthol, and methyl salicylate (wintergreen) dissolved in an alcohol base. In a stroke of marketing genius, he named the amber liquid “Listerine” in honor of the British pioneer.

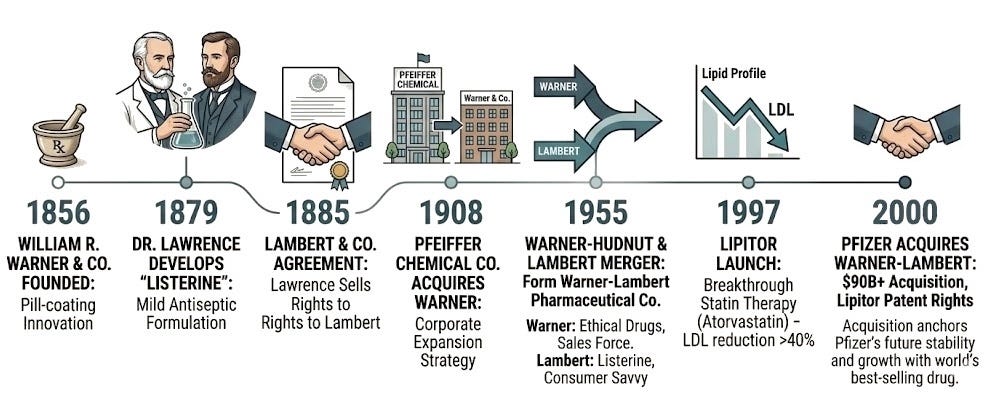
While Dr. Lawrence was a brilliant formulator, he lacked the capital and the desire to run a large-scale manufacturing enterprise. Lambert, recognizing the massive commercial potential of a safe, multi-purpose germicide, approached Dr. Lawrence to buy the rights to the formula. On April 20, 1881, the two men signed a brief, plainly worded agreement. Lawrence turned over the secret formula for Listerine to Lambert. In exchange, Lambert promised that his “heirs, executors, and assigns,” would pay a monthly royalty to Dr. Lawrence and his heirs based on gross sales. Initially set at $20 per vial, Dr. Lawrence voluntarily reduced the royalty to $12 per vial a few months later, on the condition that Lambert provide him with meticulous monthly sales statements.
The agreement had an unforeseen side effect. Decades later, long after Lambert Pharmacal had merged into Warner-Lambert (and eventually acquired by Pfizer and then Johnson & Johnson), corporate attorneys attempted to stop paying the royalties to the estate of Dr. Lawrence. They argued that because the secret formula for Listerine had been openly published in a medical journal in 1931, it was no longer a “trade secret” and the contract should be void. However, in a landmark 1959 federal court ruling (Warner-Lambert Pharmaceutical Co. v. John J. Reynolds, Inc.), the judge looked back to the original 1881 and 1885 agreements executed in St. Louis. Since Jordan W. Lambert had promised to pay royalties for “each and every gross sold” without specifying a time limit or an expiration date based on secrecy, the court ruled the contract remained valid in perpetuity. To this day, the heirs of Dr. Joseph Lawrence still receive steady, lucrative royalty payments from every single bottle of Listerine sold worldwide all because of an unyielding written formula agreement executed in the early days of Lambert Pharmacal.
Armed with the exclusive rights to Listerine, Jordan W. Lambert immediately established Lambert & Co. in 1881 to begin producing the antiseptic on a modest commercial scale. As the business steadily grew and expanded its product line to include other medical preparations (such as “Lithiated Hydrangea”), Lambert recognized the need for a formal corporate structure to protect his assets and attract broader investment. On November 13, 1885, the business was officially reorganized and incorporated as the formally named Lambert Pharmacal Company in St. Louis. To transition the business smoothly into this new entity, a second agreement was signed in 1885. Dr. Lawrence officially transferred his royalty rights from Lambert as an individual to the newly formed Lambert Pharmacal Company, reducing the royalty payment down to a sustainable $6 per gross of Listerine manufactured or sold.
In its earliest incarnation under the newly minted Lambert Pharmacal banner, Listerine was not the household mouthwash it is today. Lambert marketed the product strictly to medical professionals. Early advertisements in medical journals pitched Listerine as a universal germicide safe for cleaning surgical wounds, irrigating deep abscesses, sterilizing hospital surfaces, and treating throat infections. It wasn’t until 1895 that Lambert Pharmacal began actively marketing the compound to dentists as an oral antiseptic, laying the foundation for the massive consumer empire it would eventually become in the 1920s.
Formulation Founders of Warner-Hudnut
Separately, in Philadelphia in 1856, a young, ambitious pharmacist named William Richard Warner opened a retail drug store. Warner was not content with merely mixing powders behind a counter. He was an innovator determined to solve one of the greatest patient compliance problems of the Victorian era: the horrific, bitter taste of raw medicinal ingredients.
Warner invented a highly sophisticated tablet-coating process that utilized a rotating centrifugal pan to evenly encase harsh, bitter-tasting medications in a smooth, sweet sugar shell. This elegant innovation transformed how the public took medicine, making treatments vastly more palatable. The breakthrough was so historically significant that his original equipment eventually earned a permanent place in the Smithsonian Institution. Recognizing that the mass manufacture of these coated pills was far more lucrative than retail pharmacy, Warner gave up his storefront in 1886. He pivoted completely to industrial drug manufacturing under the name William R. Warner & Co., establishing the firm as a premier supplier of mass-produced, reliable pharmaceuticals.
While William R. Warner & Co. built its reputation on manufacturing quality and scientific innovation, its next phase of growth would be driven by raw corporate strategy. In 1901, a highly aggressive patent-medicine enterprise called the Pfeiffer Chemical Company was founded in St. Louis, Missouri, by the brothers Henry and Gustavus A. Pfeiffer. The Pfeiffers were master corporate strategists who realized that building a drug company from scratch was far slower than simply buying existing, reputable brands and optimizing their distribution networks.
In 1908, the Pfeiffer Chemical Company acquired William R. Warner & Co. Recognizing that the “Warner” name carried immense trust and prestige among doctors and pharmacists, the Pfeiffers made a calculated decision: they absorbed their own company into the acquisition, kept the William R. Warner name, and eventually moved the corporate headquarters to New York City. Under Henry Pfeiffer’s leadership, the company embarked on a decades-long buying spree, acquiring over 50 separate companies, including the legendary Richard Hudnut cosmetics and DuBarry beauty businesses. By 1950, to reflect its highly successful diversification into both beauty and drugs, the company renamed itself Warner-Hudnut.
Better Together
By the mid-1950s, the pharmaceutical industry was rapidly evolving. The post-WWII boom brought a wave of new synthetic drugs, antibiotics, and a massive rise in consumer spending. To survive, a company needed incredible scale to fund expensive Research and Development (R&D) while simultaneously bankrolling aggressive national television advertising campaigns.
Led by its sharp chief executive, Elmer Bobst (a legendary pharmaceutical executive who had previously built Hoffman-La Roche’s American business), Warner-Hudnut was highly profitable. It had a robust stable of prescription (”ethical”) drugs and a massive, lucrative cosmetics division via its Richard Hudnut line. However, Bobst recognized a glaring weakness: the company completely lacked a ubiquitous, recession-proof, everyday over-the-counter (OTC) consumer mega-brand. Its earnings were heavily dependent on the whims of fashion trends and the volatile cycle of new prescription drug discoveries.
Meanwhile, the Lambert Pharmacal Company was sitting on a mountain of cash generated by a single, cultural juggernaut: Listerine. Thanks to the legendary “halitosis” (bad breath) advertising campaigns of the 1920s and 30s, Listerine completely dominated the oral hygiene market. Yet, Lambert’s leadership knew they were dangerously over-reliant on a single product. Furthermore, while they were masters of consumer marketing, they lacked the deeply entrenched international distribution networks, the corporate infrastructure, and the chemical R&D pipelines required to successfully break into the highly lucrative field of prescription pharmaceutical research.
Elmer Bobst of Warner-Hudnut and Edward Williams (the president of Lambert) realized that a merger would instantly solve the existential vulnerabilities of both firms. On March 31, 1955, a deal was structured as a smooth, friendly stock-swap merger to form the Warner-Lambert Pharmaceutical Company. Stockholders of Lambert Pharmacal received shares of Warner-Hudnut on a one-for-one basis, and the two corporate cultures blended seamlessly. Williams became the new president of the unified firm, while the formidable Elmer Bobst took the reins as Chairman of the Board. The synergy was immediate and beautiful:
Warner-Hudnut contributed: Deep R&D pipelines for prescription drugs, global sales forces calling on hospitals/doctors, and elite international distribution channels.
Lambert Pharmacal contributed: Listerine’s massive and steady cash flows, world-class mass consumer marketing savvy, and dominance in supermarket and drugstore retail.
The creation of Warner-Lambert changed how the business community viewed healthcare companies, suggesting to contemporary analysts that a hybrid model anchored by consumer products could help offset the high-risk, high-reward financial cycles of laboratory drug discovery. This blueprint allowed Warner-Lambert to expand aggressively over the next four decades. Their combined pharmaceutical pipeline encompassed a number of medical “firsts”, powered almost entirely by Parke-Davis, a legendary drug company they acquired in 1970.
Anticonvulsant for seizures: Before the late 1930s, treatments for epilepsy were highly sedative, often leaving patients severely lethargic. In 1938, Parke-Davis commercialized Dilantin, the first widely available anti-convulsant that could successfully suppress grand mal seizures without completely knocking the patient out. Dilantin effectively allowed millions of people with epilepsy to live normal, functional lives and is still used in neurology.
Antihistamine for allergies: In 1946, Parke-Davis introduced Benadryl, the very first prescription antihistamine approved by the FDA. Discovered by chemical engineer George Rieveschl, it revolutionized the treatment of seasonal allergies and acute hives. Decades later, it transitioned to an over-the-counter juggernaut and remains one of the most recognizable, widely used allergy medications globally.
Fibrate for coronary heart disease: In 1982, they launched Lopid, a drug belonging to the fibrate class and gave Warner-Lambert’s sales force their first major foothold in the lucrative cardiology market. This was the first effective cholesterol-lowering agent, foreshadowing a future blockbuster.
Surgical Anesthetic: In 1962, Parke-Davis scientists synthesized ketamine, which they brought to market under the brand name Ketalar. It was a revolutionary advancement in emergency medicine and battlefield surgery because it acted as a “dissociative anesthetic.” Unlike traditional anesthetics, ketamine provided profound pain relief and sedation without suppressing a patient’s breathing or blood pressure, making it incredibly safe in trauma situations.
Snatching Victory from the Jaws of Pipeline Prioritization
Warner-Lambert’s R&D engine ultimately led them to develop Lipitor (atorvastatin), the world’s bestselling drug of all time (until it was surpassed by AbbVie/Abbott Lab’s Humira in 2012).
The concept of blocking cholesterol production in the liver began in the 1970s with a Japanese microbiologist named Akira Endo, working for the company Sankyo. Endo discovered that certain molds naturally produced compounds to defend themselves against microbes by blocking a critical enzyme needed to build cellular walls, the exact same enzyme (HMG-CoA reductase) that human livers use to synthesize cholesterol. Endo isolated the first statin, called compactin (mevastatin), from a fungus.
While compactin was never brought to market due to early toxicity scares in animals, the American pharmaceutical giant Merck was inspired by Endo’s discovery and isolated a similar, safer compound from a different mold. In 1987, Merck launched Mevacor (lovastatin), the world’s first commercially available statin. Merck quickly followed up with a more potent version called Zocor (simvastatin), while Bristol-Myers Squibb launched Pravachol (pravastatin). By the early 1990s, these drugs were turning into massive blockbusters, completely rewriting the treatment guidelines for cardiovascular disease.
Back at Warner-Lambert’s Parke-Davis research facility in Ann Arbor, Michigan, executives realized they were facing a commercial catastrophe. The cardiovascular market was shifting entirely toward statins, and they didn’t have one. Faced with an urgent strategic necessity, they tasked a brilliant young chemist named Dr. Bruce Roth with a high-stakes mission: synthesize an optimized statin molecule. Since Merck’s early statins were derived or modified from natural fungal ferments, Roth decided to take a completely different path. He set out to build a 100% fully synthetic statin from pure chemical building blocks.
Roth succeeded in 1985, synthesizing a complex molecule named atorvastatin. However, the corporate executive committee at Warner-Lambert was deeply discouraged. In the pharmaceutical industry, a late-to-market drug that shares a mechanism of action with existing approved therapies is colloquially referred to as a ‘me-too’ drug. The executives argued that by the time atorvastatin completed a decade of expensive clinical trials, doctors would already be deeply loyal to Zocor and Pravachol. Furthermore, early testing in animals showed that atorvastatin didn’t seem any more potent than Merck’s drugs. The project was viewed as a massive financial risk, and the committee came incredibly close to canceling Roth’s research entirely to save money.
The project survived only because a group of stubborn Parke-Davis clinical scientists begged for a budget to test the drug in human volunteers. When the human clinical data finally came back, it revealed a monumental biological surprise that changed everything: humans processed Roth’s synthetic molecule completely differently than animals. Atorvastatin possessed an incredibly long biological half-life compared to its predecessors. It stayed in the human liver far longer, continuously blocking cholesterol synthesis for hours. Other statins on the market required high doses and generally lowered “bad” LDL cholesterol by 20% to 35%. Atorvastatin knocked down LDL cholesterol by an unprecedented 40% to 60%, even at the lowest starting dose.
In classic pharmaceutical economics, being late to market with a drug in the same class is usually an insurmountable commercial hurdle. The pioneers have already locked in doctor loyalty, secured preferred status on insurance formularies, and captured market share. When Lipitor finally launched in 1997, it was officially the fifth statin approved for the global market, trailing well behind deeply entrenched titans. Nevertheless, its late-comer status didn’t matter. Backed by clinical data demonstrating significant reductions in major cardiovascular events, it quickly dethroned others and claimed the crown as the most financially successful medicine ever created.
Warner-Lambert possessed world-class consumer marketing savvy (perfected over decades of selling Listerine and Trident gum), but they knew their cardiovascular “ethical drug” sales force lacked the sheer scale required to go toe-to-toe with Merck’s mighty Zocor sales force. To overcome this, they executed a brilliant strategic maneuver before the launch, signing a co-marketing agreement with Pfizer. Pfizer boasted a formidable, aggressive, and trusted sales force. Under the terms of the deal, both companies would deploy their sales representatives to promote Lipitor, splitting its massive profits.
The Pfizer/Warner-Lambert alliance oversaw an unconventional medical marketing strategy. Instead of targeting only elite cardiologists, an army of sales representatives descended upon ordinary primary care physicians (PCPs) and family doctors. Armed with clinical data showing that Lipitor could drop “bad” LDL cholesterol by an unprecedented 40% to 60% even at its lowest starting dose, they successfully shifted the medical paradigm. They framed cholesterol management as a preventative strategy for everyday middle-aged adults, not merely as a treatment for severely ill cardiac patients. Backed by a historic wave of direct-to-consumer television and print advertisements, Lipitor achieved an unprecedented launch, crossing $1 billion in domestic sales within its first twelve months on the market. According to reported corporate financial data, the drug reached $12.9 billion peak annual sales in 2008, before its initial loss of patent exclusivity.
Big Fish, Little Fish
As Lipitor’s sales trajectory went vertical, it created an unstable corporate paradox. Pfizer was generating billions of dollars in revenue from the drug and its stock price was soaring, but they were split-marketing a molecule they did not actually own. Warner-Lambert owned the patent, and they were fiercely protective of their golden goose. The corporate arrangement was highly profitable but marked by intense strategic friction, and by 1999, the tension reached a breaking point. Recognizing that their massive success with Lipitor made them an attractive target for a hostile takeover, Warner-Lambert’s management looked for ways to insulate the company.
On November 4, 1999, Warner-Lambert stunned the business community by announcing a surprise $54 billion merger with American Home Products (AHP), a massive consumer goods and drug conglomerate. The combined entity, to be named “American Warner,” would have instantly become the largest pharmaceutical and consumer health company in the world. For Pfizer’s leadership, led by CEO William Steere, this announcement was an existential threat. If Warner-Lambert successfully merged with AHP, Pfizer risked losing its lucrative co-marketing rights on Lipitor due to change-of-control clauses, or worse, facing a massive new competitor holding the primary commercial rights to the world’s best-selling drug.
Pfizer struck back with haste. Hours after the AHP announcement, Pfizer launched an unsolicited counter-bid of $82 billion to buy Warner-Lambert directly. What followed was a highly contested three-month corporate standoff. Warner-Lambert’s board utilized standard corporate ‘poison pills’ and defense mechanisms to block Pfizer’s approach. Pfizer sued Warner-Lambert in a Delaware court, successfully arguing that the board had a fiduciary duty to let shareholders vote on Pfizer’s vastly superior financial offer. Warner-Lambert executives formally advised shareholders to support the friendly AHP merger, arguing it preserved the company’s long-term identity. Pfizer countered by steadily raising its bid, making it mathematically impossible for shareholders to refuse.
By early 2000, Pfizer’s escalating financial terms left Warner-Lambert with few viable alternatives. Facing pressure from institutional shareholders, and realizing Pfizer would not back down, Warner-Lambert’s board determined that accepting the revised proposal was in the best financial interest of its shareholders. On February 7, 2000, Warner-Lambert officially terminated its merger agreement with American Home Products. To walk away, Warner-Lambert paid AHP a record-breaking $1.8 billion breakup fee, a penalty Pfizer happily absorbed as part of the final transaction.
Pfizer increased its final purchase price to a staggering $90.2 billion in stock, completing the acquisition in June 2000, creating “the world’s most valuable and fastest-growing pharmaceutical company” at the time. It stood as the largest pharmaceutical corporate hostile takeover in history. Over its patent lifetime, Lipitor generated more than $130 billion in total revenue. For over a decade, it served as the financial engine that anchored Pfizer’s corporate stability and funded its subsequent mega-mergers (such as the acquisition of Pharmacia in 2003 and Wyeth in 2009).
The merger triggered a large-scale corporate restructuring. Warner-Lambert had been a diversified conglomerate, boasting massive consumer health, confectionery, and shaving divisions alongside its core drug portfolio. Pfizer, however, was fundamentally a pure-play pharmaceutical firm and had little interest in managing candy or razor blades. To recoup cash and refocus the business, Pfizer initiated a sale of Warner-Lambert’s iconic non-pharmaceutical brands, including Listerine.
Initially, Pfizer retained the highly lucrative consumer healthcare line. However, in 2006, Pfizer decided to exit the over-the-counter consumer space entirely, selling its consumer healthcare division, anchored heavily by Listerine, to Johnson & Johnson (J&J) for a staggering $16.6 billion. In May 2023, J&J announced their intention to spin off its entire consumer health portfolio (including Listerine, Tylenol, Band-Aid, and Neutrogena) into a brand-new, independent, publicly traded company called Kenvue Inc. By August 2023, J&J had fully divested its ownership stake, making Kenvue completely separate. Kenvue’s time as a standalone company was relatively brief. In November 2025, consumer products giant Kimberly-Clark (the maker of Huggies, Kleenex, and Scott) announced a definitive agreement to acquire Kenvue in a deal valued at an estimated $48.7 billion in cash and stock.
Through these massive divestitures, the historic Listerine products of the Lambert Pharmacal Company found a home at Kimberly-Clark, where they reside today.
Conclusion
The corporate lineage that began with a Victorian pharmacist coating bitter pills in sugar and a St. Louis doctor blending volatile plant oils in a glass flask reached an extraordinary, unforeseen destination. The trajectory of Warner-Lambert serves as a striking reminder of the grand, unpredictable nature of the biotech industry. Without the cash engine of Listerine, the world may have never seen Lipitor. Yet, it was that very same miracle molecule that ultimately painted a target on the company’s back, invoking a $90 billion hostile takeover that ultimately led to the strategic reorganization and divestiture of the conglomerate.
Today, the diverse threads of the old Warner-Lambert empire have been untangled and integrated into the bedrock of modern consumer health and big pharma. Its prescription pipeline permanently anchored Pfizer’s global dominance, while Listerine ultimately landed under the stewardship of consumer products giant Kimberly-Clark. Warner-Lambert as a corporate entity may now be a ghost, but its historical footprint is undeniable. From the battlefields of the nineteenth-century germ revolution to the structured, multibillion-dollar blockbuster dynamics of today’s medicine cabinet, its legacy survives, reminding us that while names on a corporate marquee may fade, true clinical and commercial innovations endure forever.
To contact us, please send us an email at biotechreadout@gmail.com
Disclaimers
Investigational Status Disclaimer
The therapeutic candidates discussed in this newsletter are currently in clinical development and have not been approved for commercial sale by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), or other global regulatory authorities. Their safety and efficacy have not been established. References to pipeline products and ongoing clinical trials involve significant risks and uncertainties. Statements regarding the potential safety, potency, or efficacy of investigational drugs reflect current hypotheses and are not a guarantee of future performance or regulatory clearance. The outcome of clinical trials is inherently unpredictable, and clinical results from earlier stages may not be predictive of results in later, larger-scale trials.
No Medical Advice Disclaimer
This newsletter is for informational and educational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this publication.
No Patient-Provider Relationship Disclaimer
The information provided in this newsletter is for educational and analytical purposes only. Receipt of this information, or any interaction with this content, does not create a physician-patient, pharmacist-patient, or any other professional-provider relationship between you and the authors or publishers. This newsletter should not be used as a substitute for a personal consultation with a qualified healthcare professional.
Forward-Looking Statements Disclaimer
This newsletter contains “forward-looking statements” regarding future events, including clinical trial timing, regulatory milestones, and projected market performance. These statements are based on current expectations and assumptions that are subject to significant risks and uncertainties. Actual results may differ materially from those expressed or implied. We undertake no obligation to update these statements as a result of new information or future developments.
Third-Party Links & Content Disclaimer
This newsletter contains links to third-party websites, including clinical trial registries and corporate presentations. Biotech Readout does not endorse, guarantee, or assume responsibility for the accuracy or reliability of any information offered by third-party providers.
Errors and Omissions Disclaimer
While we strive for technical accuracy, the information in this newsletter is provided on an “as is” basis with no guarantees of completeness, accuracy, or timeliness. Biotech Readout assumes no liability for any errors or omissions in the content of this publication.
Non-Endorsement Disclaimer
Any reference to specific commercial products, processes, or services by trade name, trademark, or manufacturer does not constitute or imply an endorsement or recommendation by the author. All trademarks are the property of their respective owners.
No Investment Advice Disclaimer
This newsletter is for informational purposes only and does not constitute financial, investment, or legal advice. The author is not a registered investment advisor. You should consult with a professional financial advisor before making any investment decisions. The biotechnology sector is highly volatile; past performance is not indicative of future results.
Conflict of Interest Disclaimer
The author of this newsletter maintains a position of independence. At the time of publication, the author holds no direct financial interest, equity, or options in any of the companies mentioned in this report. No compensation has been received from any third party to feature or analyze specific therapeutic candidates or corporate entities.