
United Therapeutics to Acquire Thymmune
Regenerative medicine titans join forces to grow a thymus

Disclaimer: This newsletter is for educational and informational purposes only and does not constitute medical, investment, or financial advice, nor does it establish a provider-patient relationship. Content may include forward-looking statements and discussions of investigational therapeutic candidates that are not FDA/EMA approved; their safety and efficacy remain unestablished and clinical outcomes are unpredictable. While we strive for accuracy, all information is provided as is without guarantees. As of the date of publication, the author holds no direct equity positions in the specific companies mentioned in this issue nor receives third-party compensation for this coverage. Please find a complete version of our disclaimers at the bottom of this article and on our About page.

Introduction
On July 2, 2026, United Therapeutics Corporation announced that it has acquired Thymmune Therapeutics, Inc. for $140 million in cash plus up to $160 million based on the achievement of certain clinical and regulatory milestones by the end of 2031, for a total deal value of up to $300 million. This acquisition centers on THY-100, an investigational, preclinical neo-thymus cell therapy being evaluated to treat congenital athymia (infants born without a functional thymus).
In this article, we dive into the role of stem cell reprogramming in regenerative medicine, explore how foundational work in the George Church lab led to the spinout of Thymmune, and learn how Thymmune fits into United Therapeutics’ regenerative medicine ambitions.
The Church of Cell Reprogramming
Thymmune Therapeutics traces its roots back to foundational research in George Church’s laboratory at Harvard Medical School and the Wyss Institute. A major focus of his lab is regenerative medicine, which aims to do something pharmacological medicine struggles to achieve: repair, replace, or regenerate damaged tissues and organs rather than managing disease symptoms. Stem cells are a foundational engine of this field because they possess two unique properties that make them the cellular raw material for regeneration:
Self-Renewal: The ability to divide and replicate themselves indefinitely in a lab environment, creating an inexhaustible supply of starting material.
Potency: The ability to differentiate (mature) into specialized functional cells, such as heart muscle cells, neurons, or insulin-producing pancreatic cells.
An enabling technology for the Church lab’s research is the induced pluripotent stem cell (iPSC). The process of making iPSCs was discovered in 2006 by Shinya Yamanaka (which earned him a Nobel Prize). It involves taking adult cells and introducing a specific cocktail of four master genes, known as the Yamanaka Factors (Oct3/4, Sox2, Klf4, and c-Myc). These factors wipe the cell’s memory, rewinding its developmental clock back to zero. To be clear, iPSCs are different from embryonic stem cells (ESCs). Both types of stem cells are theoretically able to differentiate into virtually any cell type in the human body, but they diverge in their origin and the ethical considerations surrounding them. Embryonic stem cells are derived directly from the inner cell mass of a pre-implantation human embryo that is typically four to five days old. This derivation process inherently results in the destruction of the embryo, which has historically sparked intense ethical, religious, and political debates worldwide, leading to strict regulatory bottlenecks. In contrast, iPSCs come from fully mature adult cells (typically skin fibroblasts or peripheral blood cells) and are genetically reprogramed back into an embryonic-like state using Yamanaka Factors.
Yet, making stem cells is half the battle. In order to craft a regenerative medicine for a particular treatment context, you need to know how to program the stem cells into the specific type of mature cell that you need. For example, you would need to make collagen-producing fibroblasts in the context of knee regeneration, but you would need to make nerve cells in the context of spine regeneration. That last mile of cell programming is where the Church lab shines. The lab uses synthetic biology and machine learning techniques to figure out how to make specific cell types from iPSCs. By utilizing pooled screens of transcription factors, researchers in the lab systematically identified the master switches required to convert induced pluripotent stem cells (iPSCs) directly into highly specialized cell types.
Their 2020 Nature Biotechnology paper entitled “A comprehensive library of human transcription factors for cell fate engineering” was a major advance in the field of regenerative medicine. Traditional stem cell differentiation relied on recreating natural, slow, and expensive embryonic signaling pathways using chemical morphogens in specialized lab environments. The Church lab bypassed this developmental path by focusing entirely on transcription factors, the master genetic switches that control cell identity. By executing massive pooled genetic screens on human induced pluripotent stem cells (hiPSCs), the team identified 290 distinct transcription factors capable of driving stem cells to differentiate into mature target cells within just 4 days. Remarkably, 241 of these TFs were previously entirely unreported to possess cell-fate capabilities. The researchers validated their screening hits by programming stem cells into high-quality, fully functional adult tissue lineages that matched primary human tissue control profiles. The paper specifically demonstrated four distinct lineages:
Neurons & Fibroblasts: The team derived functional neurons that displayed proper electrophysiological patch-clamp readings and fibroblasts that successfully healed an in vitro wound-scratch monolayer.
Vascular Endothelial Cells: Utilizing a specific splice variant (ETV2 isoform 2), they achieved nearly 100% differentiation efficiency into endothelial-like cells that successfully formed functional, perfusable blood vessels integrated with host circulatory systems in vivo.
Oligodendrocytes: They co-cultured engineered, oligodendrocyte-inducible hiPSCs alongside unmodified hiPSCs to generate complex cerebral organoids. This allowed different cell types to mature synchronously, radically accelerating in situ myelination of axons.
Ultimately, the Church lab’s Human TFome project wrote the rules of cell reprogramming. The ability to program induced pluripotent stem cells (iPSCs) rapidly and autonomously provided the means to mass-produce complex, therapeutic tissues, setting the stage for spinouts like Thymmune to engineer a functional neo-thymus in vivo.
Growing a Thymus
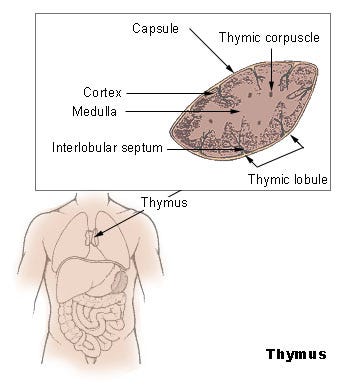
The thymus is a small organ located behind your breastbone, and it acts as the training ground for the immune system. It takes immature immune cells from the bone marrow and teaches them to become T-cells, the specialized soldiers that fight off viruses, bacteria, and cancer. Unfortunately, this crucial organ is not as resilient as it ought to be.
{kind=link}
Unlike almost every other organ, the thymus begins to shrink and turn to fat starting at puberty. By the time you reach old age, your thymus is operating at a fraction of its capacity. This is a primary reason why older adults are far more vulnerable to new infections (like COVID-19 or influenza) and why their bodies are less effective at clearing emerging cancer cells. Patients with congenital athymia, a rare genetic condition where children are born entirely without a thymus, cannot produce T cells, leaving them with a severely weakened immune system. Historically, the condition is fatal within the first two years of life without an intervention.
If you want to fix an organ using a regenerative medicine approach with embryonic stem cells (ESCs), you could take a stem cell and expose it to a sequence of chemical growth factors (morphogens) that mimic human embryonic development. However, growing Thymic Epithelial Cells (TECs) was particularly challenging for three reasons:
The Complexity of the Epithelial Scaffold: The thymus isn’t just a collection of loose cells. It is a highly intricate, three-dimensional physical meshwork. As immature T-cells crawl through this biological maze, TECs must physically touch them to present self-antigens. This teaches the T-cells two things: how to recognize foreign invaders (positive selection) and how not to attack your own body (negative selection). Replicating this complex, interactive 3D behavior in a flat plastic dish using standard chemical signaling had proven nearly impossible.
High Instability and Loss of Identity: When researchers did manage to isolate primary thymic epithelial cells from tissue donors, they encountered a major hurdle: the moment these cells were cultured outside the body, they rapidly lost their functional identity in a process called dedifferentiation. Within a few cell divisions, they ceased expressing the critical genes, like FOXN1 (the master regulator of thymic development), needed to train T-cells.
The Yield Problem: Since the differentiation pathways are so convoluted, traditional methods resulted in horribly low yields. You might end up with a tiny fraction of functional cells hidden among a mess of chaotic, half-differentiated tissues. To treat a patient, doctors need hundreds of millions of highly pure, synchronized cells.
The George Church lab’s Human TFome project gave scientists much higher agency in making Thymic Epithelial Cells (TECs) from iPSCs. The actual translation of this platform specifically into the thymic lineage was driven by Stan Wang, during and immediately following a postdoctoral fellowship in the Church lab. Rather than publishing the specific iPSC-to-TEC cocktail in an open-access academic paper, the specialized genetic recipes, machine learning optimization algorithms, and methods for forming a functional neo-thymus in vivo were largely protected as proprietary intellectual property and patent filings. This proprietary execution of the Church lab’s screening methodology became the foundation upon which Wang spun out Thymmune Therapeutics in 2019.
The company established its operations in Kendall Square in 2021 and immediately captured the interest of major pharmaceutical players. That year, Thymmune won five “Golden Tickets” from major sponsors including Pfizer, Novo Nordisk, LG Chem Life Sciences, Boehringer Ingelheim, and Astellas. These awards equipped the fledgling company with critical early industry validation and lab space. Thymmune formally launched out of stealth in March 2023, securing a $7 million seed financing round led by Pillar VC, with participation from New York Blood Center’s NYBC Ventures, George Church, and former Alnylam CEO John Maraganore. The corporate trajectory accelerated significantly in September 2023, when Thymmune became one of the very first industry projects funded by the Biden administration’s newly formed Advanced Research Projects Agency for Health (ARPA-H). The agency awarded Thymmune up to $37 million under its Open Broad Agency Announcement to fund its “Thymus Rejuvenation” project. This non-dilutive capital gave Thymmune an immense runway to build out its infrastructure across two parallel validation phases:
Phase 1: Utilizing human induced pluripotent stem cell-derived thymic epithelial cells (iPS-TECs) to restore T-cell development in thymus-incompetent animals and slow immunologic aging.
Phase 2: Scaling up the manufacturing process for transplantation models to establish a viable clinical pathway.
With strong financial backing, leadership expanded the executive layer, bringing on veteran biopharma talent including Chief Scientific Officer Bing Lim, and Chief Technology Officer Manish Jain. The team directed their machine learning platform toward industrializing the production of off-the-shelf, scalable iPSC-derived thymic cells. The buildout centered heavily on THY-100, the company’s lead preclinical candidate for congenital athymia (infants born without a functional thymus). In animal models, Thymmune demonstrated that a less-invasive injection of their engineered cells could induce in vivo self-assembly, forming a functional, vascularized neo-thymus capable of facilitating independent T-cell development in these models. Beyond athymia, the company scaled its research into broader horizons, targeting age-related immune decline and post-transplant organ tolerance.
The rapid buildout of Thymmune’s platform culminated in a major consolidation of the regenerative medicine space. On July 2, 2026, Thymmune was acquired by United Therapeutics, a company that is not a stranger to regenerative medicine. Driven by CEO Martine Rothblatt’s mission to solve the global organ shortage, the company’s alternative organ pipeline is organized across three scientific pillars:
Xenotransplantation: Xenotransplantation relies on genetic engineering to strip porcine (pig) organs of the carbohydrate molecules that trigger hyperacute human immune rejection, turning them into immediate, viable alternatives for human transplant. They are developing UHeart for end-stage heart disease, UKidney for end-stage renal disease, and UThymoKidney to solve the problem of post-transplant rejection (the goal is to the train the patient’s recipient T-cells to recognize the foreign organ as self).
Allogeneic Bioengineered Organs: Acquired by United Therapeutics for over $100 million, the Miromatrix subsidiary bypasses gene-editing by leveraging a unique perfusion decellularization and recellularization technology. Scientists take an off-the-shelf porcine organ and use a specialized chemical wash to strip away all animal cells, leaving behind an intact, pristine, non-immunogenic three-dimensional collagen scaffold. This scaffold is seeded (recellularized) with human vascular and organ-specific cells. They are starting with an external liver assist product, which is similar to dialysis for liver failure.
Autologous iPSC Regenerative Medicine: The long-term holy grail of United Therapeutics’ pipeline is to completely eliminate human immune rejection by utilizing a patient’s own cells or universal, stealth cellular lines to manufacture personalized tissue. Here, they are starting with ULung and ULobe for end-stage lung disease. Developed through partnerships with 3D-bioprinting leaders like 3D Systems, this program prints complex, high-resolution synthetic lung scaffolds embedded with patient-derived or highly compatible human stem cells. The long-term developmental goal is to construct a fully functioning, cellularized human lung capable of independent gas exchange. The Thymmune acquisition falls squarely into this bucket.
Conclusion
The acquisition of Thymmune by United Therapeutics represents a textbook synergy between academic innovation and industry acceleration. The foundational work emerging from the George Church lab provided its enabling technology: a method for using transcription factors to orchestrate cellular reprogramming. Nevertheless, turning a brilliant academic insight into a scalable cell therapy requires a completely different set of capabilities. It demands the refinement of experiments into repeatable & scalable processes, the navigation of complex regulatory frameworks, and a long financial runway. By absorbing Thymmune, United Therapeutics is integrating a sophisticated cellular programming platform into their broader organ-manufacturing apparatus. Together, they hope to manifest their shared dream of engineering functional, patient-specific organs in vivo.
Love biotech? Check out Biotech Readout’s full content library, or navigate directly to a segment that interests you:
Frontiers in Medicine: Exploring the frontiers of our understanding and treatments for disease.
Medical History: Recovering forgotten relics in the history of medicine.
Acquisitions: Exploring the innovation behind acquired companies.
Weekly Readout: A digest of new clinical data from the past week.
To contact us, please send us an email at biotechreadout@gmail.com
Disclaimers
Investigational Status Disclaimer
The therapeutic candidates discussed in this newsletter are currently in clinical development and have not been approved for commercial sale by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), or other global regulatory authorities. Their safety and efficacy have not been established. References to pipeline products and ongoing clinical trials involve significant risks and uncertainties. Statements regarding the potential safety, potency, or efficacy of investigational drugs reflect current hypotheses and are not a guarantee of future performance or regulatory clearance. The outcome of clinical trials is inherently unpredictable, and clinical results from earlier stages may not be predictive of results in later, larger-scale trials.
No Medical Advice Disclaimer
This newsletter is for informational and educational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this publication.
No Patient-Provider Relationship Disclaimer
The information provided in this newsletter is for educational and analytical purposes only. Receipt of this information, or any interaction with this content, does not create a physician-patient, pharmacist-patient, or any other professional-provider relationship between you and the authors or publishers. This newsletter should not be used as a substitute for a personal consultation with a qualified healthcare professional.
Forward-Looking Statements Disclaimer
This newsletter contains “forward-looking statements” regarding future events, including clinical trial timing, regulatory milestones, and projected market performance. These statements are based on current expectations and assumptions that are subject to significant risks and uncertainties. Actual results may differ materially from those expressed or implied. We undertake no obligation to update these statements as a result of new information or future developments.
Third-Party Links & Content Disclaimer
This newsletter contains links to third-party websites, including clinical trial registries and corporate presentations. Biotech Readout does not endorse, guarantee, or assume responsibility for the accuracy or reliability of any information offered by third-party providers.
Errors and Omissions Disclaimer
While we strive for technical accuracy, the information in this newsletter is provided on an “as is” basis with no guarantees of completeness, accuracy, or timeliness. Biotech Readout assumes no liability for any errors or omissions in the content of this publication.
Non-Endorsement Disclaimer
Any reference to specific commercial products, processes, or services by trade name, trademark, or manufacturer does not constitute or imply an endorsement or recommendation by the author. All trademarks are the property of their respective owners.
No Investment Advice Disclaimer
This newsletter is for informational purposes only and does not constitute financial, investment, or legal advice. The author is not a registered investment advisor. You should consult with a professional financial advisor before making any investment decisions. The biotechnology sector is highly volatile; past performance is not indicative of future results.
Conflict of Interest Disclaimer
The author of this newsletter maintains a position of independence. At the time of publication, the author holds no direct financial interest, equity, or options in any of the companies mentioned in this report. No compensation has been received from any third party to feature or analyze specific therapeutic candidates or corporate entities.