
UCB to Acquire Candid
Scooping a reverse merger for a TCE pipeline

Disclaimer: This newsletter is for educational and informational purposes only and does not constitute medical, investment, or financial advice, nor does it establish a provider-patient relationship. Content may include forward-looking statements and discussions of investigational therapeutic candidates that are not FDA/EMA approved; their safety and efficacy remain unestablished and clinical outcomes are unpredictable. While we strive for accuracy, all information is provided as is without guarantees. This newsletter is independent, and the author holds no financial positions in the companies mentioned nor receives third-party compensation for this coverage. Revenue run rates are estimates based on the author’s synthesis of publicly available 10-K/10-Q filings and may not reflect GAAP-certified annual totals. Please find a complete version of our disclaimers at the bottom of this article and on our About page.

Introduction
On May 3, 2026, UCB announced a definitive agreement to acquire Candid Therapeutics for $2 billion upfront payments and up to $200 million in potential future milestone payments ($2.2 billion total) (UCB press release, Candid press release). The acquisition centers on four T-cell engagers (TCE) for autoimmune diseases:
Cizutamig (BMCA x CD3 TCE) / Phase 2 ready for generalized myasthenia gravis (gMG), two autoimmune disease caused by auto-antibodies that mistakenly attack the patient’s own body
CND261 (CD20 x CD3 TCE) / Phase 1
CND319 (CD19 x CD20 x CD3) / IND-enabling
CND460 (BMCA x CD19 x CD3) / IND-enabling
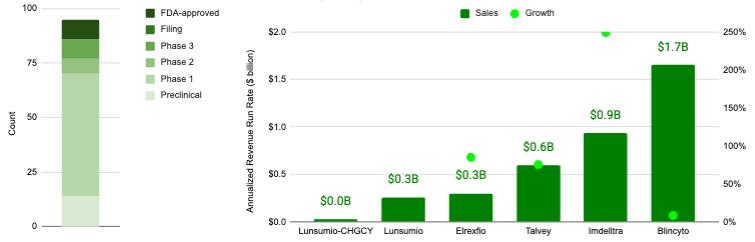
T-cell engagers (TCE) constitute a blockbuster indication space, representing an aggregate revenue run rate of almost $3.8 billion as of 4Q 2025 according to quarterly press releases associated with Blincyto, Imdelltra, Talvey, Elrexfio, and Lunsumio* (see graph below). There are only 6 approved TCE’s (recently-approved Lynozyfic doesn’t have any reported sales and isn’t pictured below), but the space is quickly becoming crowded with at least 86 clinical/preclinical programs in development.
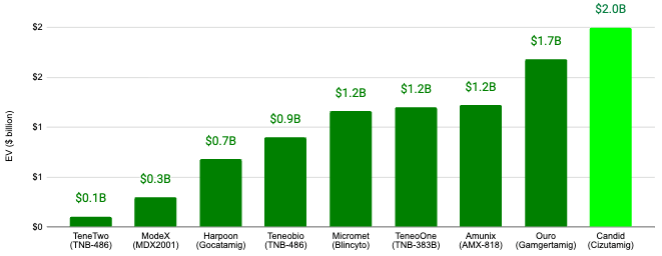
If executed, the proposed Candid acquisition would constitute the largest acquisition in the TCE space to date (see graph below).
Here, we will define how the T-cell engagers (TCE) drug modality can treat autoimmune diseases and dive into the history of Candid Therapeutics.
Teaser alert: I’m keeping this article more brief that I had originally planned because I’m working on an expansive three-part “Frontiers in Medicine” series on T-cell Therapies, which will include the history of TCEs. So, stay tuned for that!
What is a T-cell Engager (TCE)?
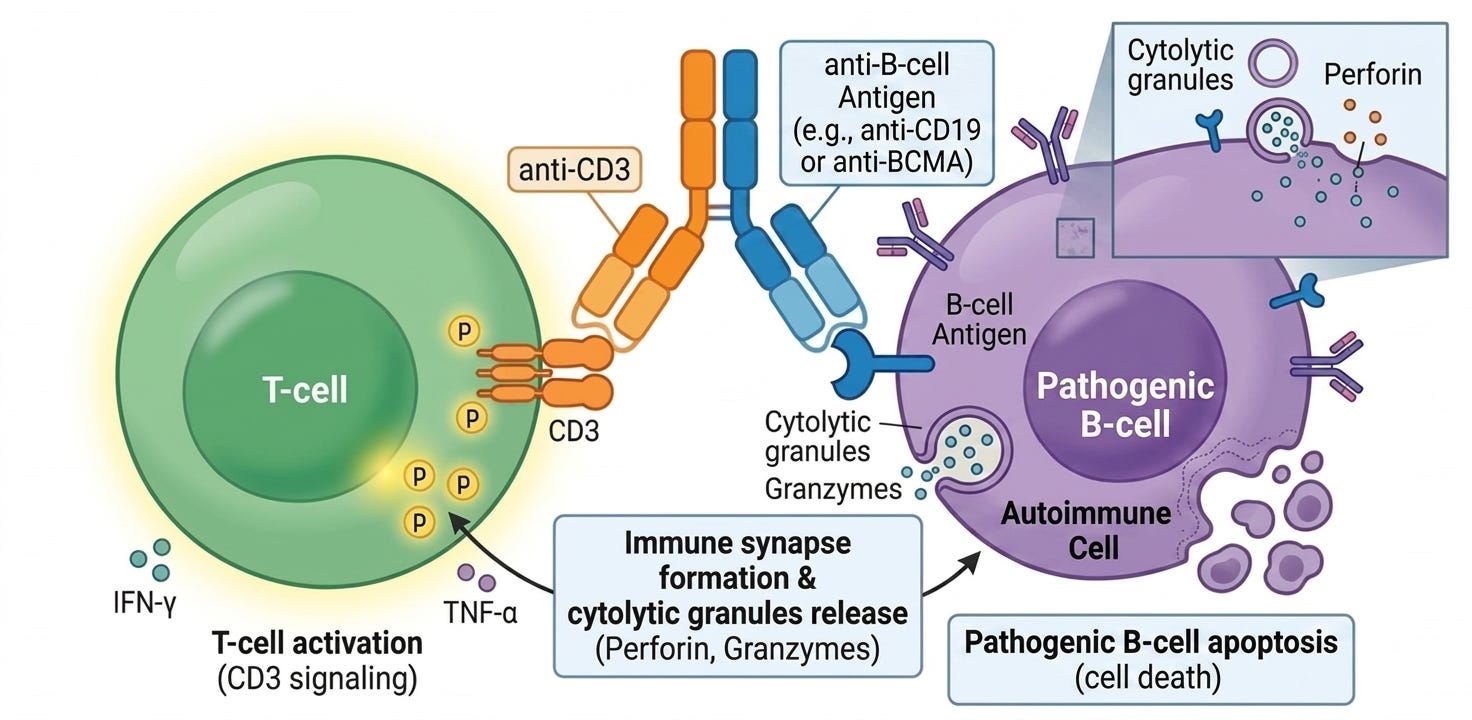
T-cell engagers (TCEs) are specialized types of immunotherapies, typically bispecific antibodies, designed to bridge the gap between a patient’s immune system and a target cell (usually a cancer cell or a pathogenic B-cell). Unlike traditional antibodies that simply flag a target for destruction, a TCE act as a molecular matchmaker: it physically grabs a T-cell and pulls it into direct contact with the target cell to force an immune attack.
A T-cell engager has two distinct binding arms:
The Effector Arm (anti-CD3): This arm binds to the CD3 receptor on the surface of a T-cell. This binding bypasses the normal, complex “recognition” process of the immune system and essentially “hot-wires” the T-cell into an active state.
The Target Arm (BCMA, CD19, and PSMA are the most common): This arm binds to a specific protein found on the surface of the cell you want to kill.
By bringing these two cells into close proximity, the TCE creates an artificial synapse. The T-cell then releases toxic enzymes (perforins and granzymes) that punch holes in the target cell, causing it to die.
Normally, T-cells only attack targets that are presented to them in a very specific way (via MHC). TCEs bypass this requirement, meaning they can kill cells that have evolved to hide from the natural immune system. Because they directly activate T-cells, they are incredibly powerful. However, this power can lead to Cytokine Release Syndrome (CRS), a firestorm of immune activity that can be dangerous if not managed. Unlike CAR-T cell therapy, which requires a bespoke, month-long manufacturing process using a patient’s own cells, TCEs are off-the-shelf drugs that can be administered immediately to any patient.
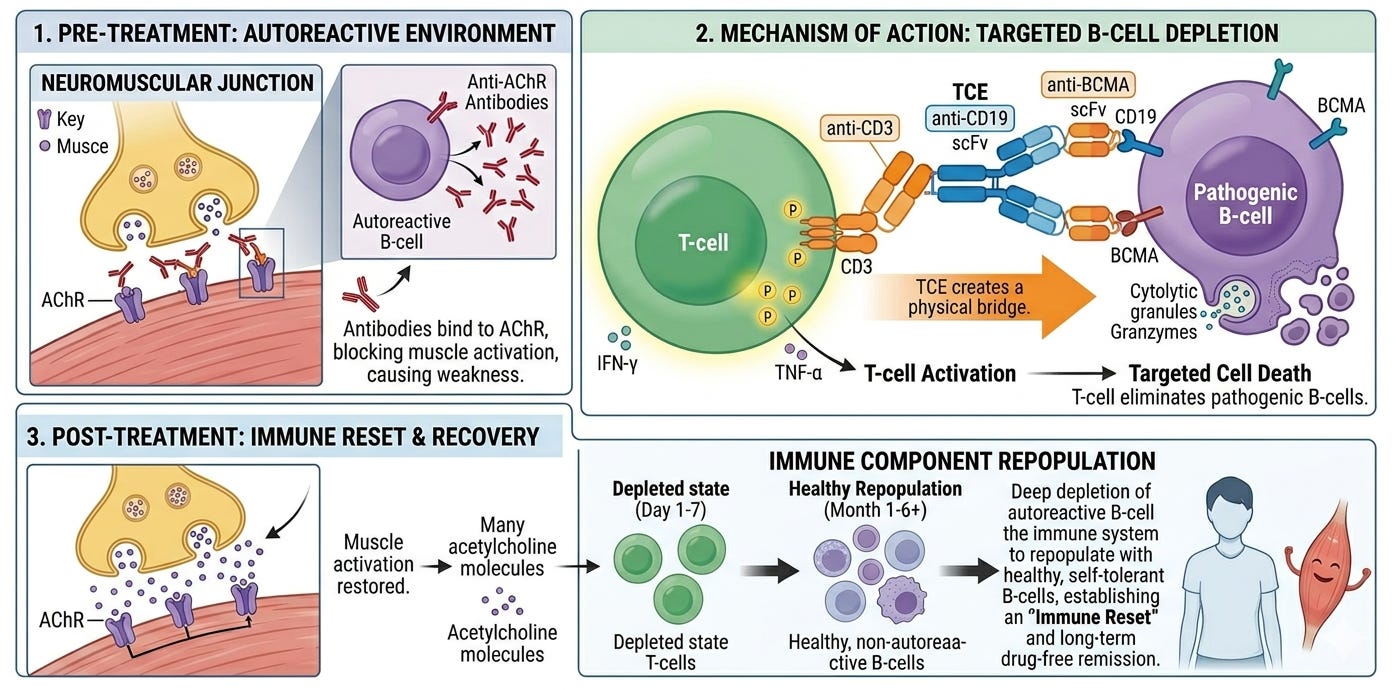
T-cell engagers (TCEs) potentially offer a potent immune reset strategy for autoimmune diseases like generalized myasthenia gravis (gMG) by mimicking the profound B-cell and plasma cell depletion observed in early CAR-T clinical trials. While traditional biologics often only partially reduce circulating B-cells, data from CAR-T therapies, such as those targeting CD19, have shown that near-complete elimination of the B-cell lineage can lead to drug-free remission for up to 2 years in lupus patients by clearing the autoantibodies at their source (see graphic below). TCEs achieve a similar depth of depletion by physically bridging endogenous T-cells to these pathogenic B-cells and long-lived plasma cells, inducing a rapid, systemic purge of the autoantibody-producing machinery. This reset allows the immune system to eventually repopulate with a naive, non-autoreactive B-cell repertoire, offering the potential for long-term clinical durability without the complex manufacturing and intensive lymphodepletion required for CAR-T. The strategic emphasis on BCMA in Candid’s cizutamig provides a unique competitive edge. Unlike CD20, which is absent on long-lived plasma cells, BCMA is highly expressed on these antibody factories. By targeting BCMA, cizutamig is designed to deplete the source of autoantibody production that remains untouched by rituximab and other CD20-targeted therapies.
Keeping it Candid
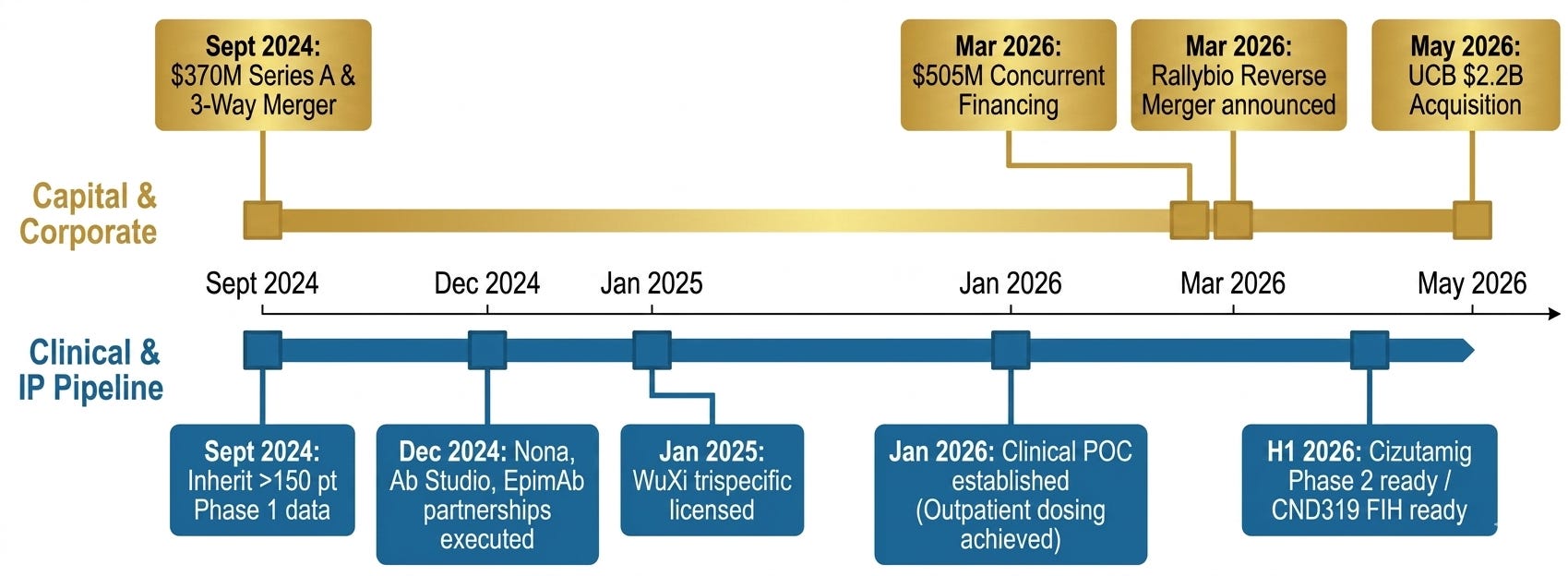
The history of Candid Therapeutics is a masterclass in the Asset Aggregator business model, comprised of a pipeline of in-licensed fast-followers drugs, moving from inception to a multi-billion dollar exit in roughly two years. Founded in September 2024, the company was built on the thesis that T-cell engagers (TCEs), which have revolutionized blood cancer treatment, could be repurposed to reset the immune system in autoimmune diseases.
Candid did not start with a single in-house discovery. Instead, it was formed through a sophisticated three-way merger and licensing strategy designed to consolidate the best available TCE assets. Candid was launched in San Diego in 2024 by proven operators:
Chief Executive Officer (CEO) Dr. Ken Song was the former CEO of RayzeBio (lead program was an actinium radiopharm targeting SSTR2 to treat GEP-NETs) and had sold it to Bristol-Myers Squibb for $4.1 billion earlier that year in February 2024
Chief Financial Officer (CFO) Arvind Kush was also CFO of RayzeBio through its IPO and sale.
Chief Medical Officer (CMO) Tim Lu, MD, PhD was previously CMO of a separate acquisition; DICE Therapeutics (oral IL-17 inhibitors for plaque psoriasis) was sold to Eli Lilly for approximately $2.4 billion in an all-cash deal in August 2023.
The company debuted with a massive $370 million capital raise led by Venrock, Fairmount, TCGX, venBio Partners. Candid simultaneously acquired Vignette Bio and TRC 2004. Through these deals, they secured the rights to their lead assets:
From Vignette: This in-housed cizutamig (BMCA x CD3 TCE), which was originally licensed from EpimAb Biotherapeutics.
From TRC 2004: This brought in CND261 (CD20 x CD3 TCE), which was originally licenced from Ab Studio.
Trispecific TCEs CND319 (CD19 x CD20 x CD3) and CND460 (BMCA x CD19 x CD3) were later in-licensed from WuXi Biologics on January 6, 2025 for up to $925 million in upfront payments, and development and sales milestones.
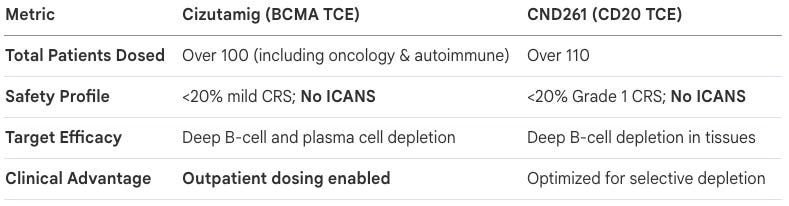
By January 2026, Candid delivered initial descriptive analysis of Phase 1 clinical data for Cizutamig and CND261 suggesting that potentially competitive profiles. While sparse, their press release described “on-target efficacy” (“B-cell/plasma cell depletion”) and “favorable safety profiles” (CRS rates with no ICANS). These molecules were optimized for an improved safety profile from the start. Cizutamig was purposely designed to prioritize T-cell mediated cytotoxicity against target cells while strictly limiting systemic cytokine production, and CND261 was developed with an engineered low CD3 affinity to prevent the over-activation of T-cells that typically drives high-grade CRS.
Importantly, Candid outlined plans to initiate Phase 2 proof-of-concept trials in two autoimmune indications (revealed to be gMG and ILD in a subsequent press release), and reported “ongoing clinical evaluation in ten [additional] indications [to] inform additional Phase 2 clinical development plans”, thereby providing additional strategic opportunities for value creation.
In early 2026, Candid attempted a rapid entry into the public markets, announcing a definitive merger agreement with the struggling public company Rallybio. The primary catalyst for Rallybio’s decline was the failure of RLYB212, its most advanced clinical candidate. It was being developed to prevent FNAIT (fetal and neonatal alloimmune thrombocytopenia), a rare bleeding disorder in newborns. In a Phase 2 trial, the drug failed to reach target concentration levels required for efficacy. The pharmacokinetic (PK) performance, and the company was forced to discontinue the entire program. With a dwindling cash runway and no late-stage clinical catalyst to attract new investors, the reverse merger with Candid, which had a high-demand pipeline and fresh capital, was a financial survival mechanism for Rallybio’s remaining shareholders.
In tandem with the reverse merger with Rallybio, Candid secured an additional $505 million in private investment (PIPE) from a syndicate including Viking Global and other investors, which would have given the combined company nearly $1 billion in cash. However, that reverse merger will never take place. In a dramatic turn of events it was superseded by a direct acquisition from a global pharmaceutical giant, UCB. UCB was already a leader in immunology and moved to preempt the IPO/merger to gain full control of cizutamig, which they believe is a “potential best in class BCMA TCE for autoimmune diseases”.
Conclusion
The acquisition of Candid Therapeutics by UCB marks a definitive end to the company’s brief but high-octane independent run, but it’s just the beginning for the TCE-in-autoimmune story. By scooping the reverse merger, UCB has just bought a pipeline that buys them time in a race where first- or best-in-class immune reset could define the next century of immunology.
Stay tuned for our upcoming three-part “Frontiers in Medicine” series on T-cell Therapies where we’ll dive deeper into their history (including antibodies, CAR-T, TCE) and explore how they have evolved from cancer-killer to autoimmune-resetter.
To contact us, please send us an email at biotechreadout@gmail.com
Disclaimers
*Revenue run rates are estimates based on the author’s synthesis of publicly available 10-K/10-Q filings and may not reflect GAAP-certified annual totals.
Investigational Status Disclaimer
The therapeutic candidates discussed in this newsletter are currently in clinical development and have not been approved for commercial sale by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), or other global regulatory authorities. Their safety and efficacy have not been established. References to pipeline products and ongoing clinical trials involve significant risks and uncertainties. Statements regarding the potential safety, potency, or efficacy of investigational drugs reflect current hypotheses and are not a guarantee of future performance or regulatory clearance. The outcome of clinical trials is inherently unpredictable, and clinical results from earlier stages may not be predictive of results in later, larger-scale trials.
No Medical Advice Disclaimer
This newsletter is for informational and educational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this publication.
No Patient-Provider Relationship Disclaimer
The information provided in this newsletter is for educational and analytical purposes only. Receipt of this information, or any interaction with this content, does not create a physician-patient, pharmacist-patient, or any other professional-provider relationship between you and the authors or publishers. This newsletter should not be used as a substitute for a personal consultation with a qualified healthcare professional.
Forward-Looking Statements Disclaimer
This newsletter contains “forward-looking statements” regarding future events, including clinical trial timing, regulatory milestones, and projected market performance. These statements are based on current expectations and assumptions that are subject to significant risks and uncertainties. Actual results may differ materially from those expressed or implied. We undertake no obligation to update these statements as a result of new information or future developments.
Third-Party Links & Content Disclaimer
This newsletter contains links to third-party websites, including clinical trial registries and corporate presentations. Biotech Readout does not endorse, guarantee, or assume responsibility for the accuracy or reliability of any information offered by third-party providers.
Errors and Omissions Disclaimer
While we strive for technical accuracy, the information in this newsletter is provided on an “as is” basis with no guarantees of completeness, accuracy, or timeliness. Biotech Readout assumes no liability for any errors or omissions in the content of this publication.
Non-Endorsement Disclaimer
Any reference to specific commercial products, processes, or services by trade name, trademark, or manufacturer does not constitute or imply an endorsement or recommendation by the author. All trademarks are the property of their respective owners.
No Investment Advice Disclaimer
This newsletter is for informational purposes only and does not constitute financial, investment, or legal advice. The author is not a registered investment advisor. You should consult with a professional financial advisor before making any investment decisions. The biotechnology sector is highly volatile; past performance is not indicative of future results.
Conflict of Interest Disclaimer
The author of this newsletter maintains a position of independence. At the time of publication, the author holds no direct financial interest, equity, or options in any of the companies mentioned in this report. No compensation has been received from any third party to feature or analyze specific therapeutic candidates or corporate entities.