
Servier to Acquire Edgewise's Muscular Dystrophy Medicine
A contrarian bet on skeletal myosin pays off

Disclaimer: This newsletter is for educational and informational purposes only and does not constitute medical, investment, or financial advice, nor does it establish a provider-patient relationship. Content may include forward-looking statements and discussions of investigational therapeutic candidates that are not FDA/EMA approved; their safety and efficacy remain unestablished and clinical outcomes are unpredictable. While we strive for accuracy, all information is provided as is without guarantees. This newsletter is independent, and the author holds no financial positions in the companies mentioned nor receives third-party compensation for this coverage. Please find a complete version of our disclaimers at the bottom of this article and on our About page.

Introduction
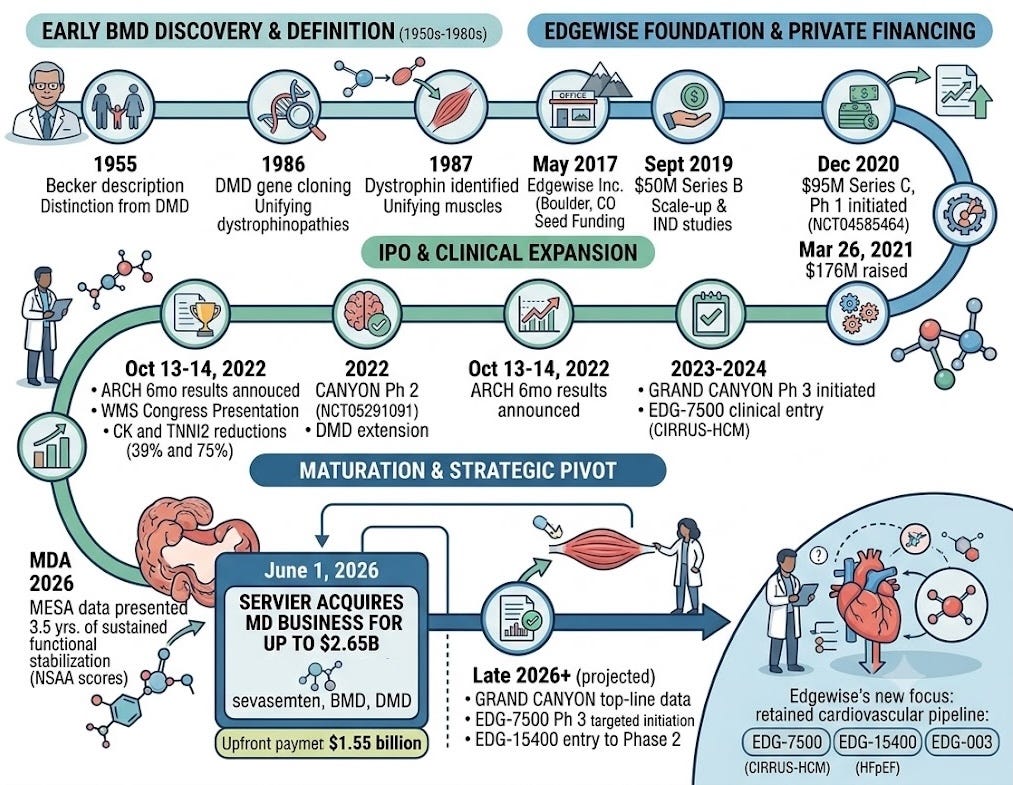
On June 1, 2026, the French pharmaceutical giant Servier announced that it has entered into an agreement to acquire the muscular dystrophy business of Edgewise Therapeutics Inc. for up to $2.65 billion, including upfront payment of $1.55 billion as well as up to $1.1 billion in regulatory and commercial milestone payments (Servier press release, Edgewise press release). At the heart of the deal is sevasemten, an orally administered fast skeletal myosin inhibitor, with a projected Phase 3 Becker Muscular Dystrophy (BMD) data readout anticipated in late 2026. Kevin Koch, Ph.D., President and CEO of Edgewise Therapeutics remarked that the deal is about, “placing sevasemten with an acquirer that has the global scale, patient commitment, and commercial reach to maximize its potential.” Rather than incurring the heavy commercialization expenses of launching an orphan drug independently, the company handed off the late-stage global execution to Servier’s established neurological infrastructure.
The $1.55 billion upfront payment almost quadruples Edgewise’s cash and equivalents in a single stroke (was $499 million in March 2026), capitalizing their transition into a cardiovascular focused company with the following pipeline:
EDG-7500 (a novel cardiac sarcomere modulator for Hypertrophic Cardiomyopathy): This is positioned to become Edgewise’s lead asset upon completion of the muscular dystrophy business divestment. It is currently anticipated to report 12-week data from Part D of the CIRRUS-HCM trial in the second quarter of 2026. This data, covering both obstructive (oHCM) and non-obstructive (nHCM) patients, will inform the Phase 3 design, which is anticipated to start in the fourth quarter of 2026.
EDG-15400 (a novel cardiac sarcomere modulator for HFpEF): Projected to enter Phase 2 later in 2026, targeting heart failure with preserved ejection fraction.
EDG-003: A preclinical asset targeting an undisclosed cardiometabolic indication.
Here, we explore how Alan Russell started Edgewise Therapeutics, how sevasemten was developed, and the history of Becker Muscular Dystrophy (BMD).
Alan Russell Flexes His Entrepreneurial Muscle
Edgewise Therapeutics emerged directly from the core muscle-biology research and industry experience of Alan Russell, Ph.D., who co-founded the company in 2017 and serves as its Chief Scientific Officer (CSO). Before co-founding Edgewise, Dr. Russell spent nearly two decades defining the biophysics of muscle contraction and therapeutic intervention.
He was a foundational scientist at Cytokinetics, where he co-invented tirasemtiv and reldesemtiv, small molecules designed to amplify muscle contractility for conditions like ALS. He was subsequently recruited by GlaxoSmithKline (GSK) to serve as Vice President and Head of the Muscle Metabolism Discovery Performance Unit. At GSK, Russell managed a massive global infrastructure dedicated to uncovering therapeutic interventions for patients with severely compromised muscle function. However, big pharma pipelines often favor broad metabolic approaches or mainstream modalities (like gene therapy and anti-inflammatories) when addressing rare neuromuscular diseases.
By 2017, Russell decided to step away from his executive track at GSK. He saw room for improvement in how the industry was addressing dystrophies like Duchenne (DMD) and Becker (BMD). The prevailing drug development consensus focused heavily on restoring missing proteins or suppressing downstream inflammation. Russell wanted to target the upstream mechanical root cause: contraction-induced microdamage. Since dystrophic muscle fibers lack structural integrity, every ordinary contraction tears them apart. Russell’s hypothesis was that a highly selective, low-affinity fast skeletal myosin inhibitor could act as a mechanical “shock absorber,” potentially easing the stress on the fibers without paralyzing the patient. Realizing that this highly specialized, mechanics-first approach required an agile, single-purpose vehicle, Russell left corporate pharma to build a platform from scratch.
Russell’s move solidified when he partnered with key venture and operational architects to turn the biophysical thesis into a viable company. He teamed up with Peter Thompson, M.D. (a Partner at OrbiMed) and Badreddin Edris, Ph.D. (an investment professional at OrbiMed and later co-founder of SpringWorks). Edgewise Therapeutics was incorporated in May 2017. OrbiMed provided the initial seed capital and they chose Boulder, Colorado as the operating base, a location deliberately selected to leverage the deep pool of muscle-biology expertise concentrated at the University of Colorado Boulder. During this initial launch phase, they established the foundational chemical platform and the core skeletal muscle thesis.
Once the early scientific groundwork was laid and the company was ready to scale toward formal asset discovery and clinical development, the board appointed Kevin Koch, Ph.D. (co-founder of Array BioPharma, which was acquired by Pfizer for $11.4 billion in 2019) as CEO. Dr. Koch’s proven track record in Colorado’s biotech ecosystem, specifically his experience as the co-founder and former CSO of Boulder-based Array BioPharma, was strategically brought in to transition Edgewise from an early-stage startup into an operational, clinical-stage company.
From there, Edgewise built a robust institutional investor base through heavily oversubscribed venture rounds to fund its lead skeletal program, sevasemten (EDG-5506), a selective fast skeletal myosin inhibitor. In September 2019, Edgewise closed a $50 million Series B financing round, co-led by Novo Holdings A/S and U.S. Venture Partners (USVP). The primary objective of the Series B capital was to scale up manufacturing, complete IND-enabling toxicology studies, and finalize the transition of sevasemten from an optimized benchtop compound into a stable, orally bioavailable clinical candidate for Becker (BMD) and Duchenne (DMD) muscular dystrophies.
With $50 million in the bank, Alan Russell and his scientific team built out a highly specialized, proprietary screening platform. Traditional high-throughput screening (HTS) in biopharma typically measures simple biochemical bindings or basic cellular viability. Edgewise had to build something much more complex: a functional muscle-biomechanics platform. The team engineered micro-physiological systems (including in vitro engineered human muscle tissues) that could simulate the precise mechanical strains experienced by a dystrophic muscle during physical contraction. During this window, the company solidified its translational strategy by mapping out downstream mechanical injury biomarkers, specifically Fast Skeletal Muscle Troponin I (TNNI2). They demonstrated in preclinical models that protecting the sarcolemma (cell membrane) from tearing resulted in an immediate, sharp drop in this structural protein’s leakage, giving them a clear biomarker scorecard to use in future human trials.
Their functional muscle-biomechanics platform was crucial for reasons that go beyond identifying development candidates that hit skeletal myosin. Russell’s allosteric skeletal myosin modulators needed to be finely tuned because they needed to overcome the toxicity of non-selective skeletal myosin inhibitors. Blebbistatin, discovered in 2003, is an allosteric inhibitor of myosin II. In a laboratory petri dish, it is incredibly effective at stopping cellular and muscle contraction. However, blebbistatin is a notoriously poorly behaved chemical tool. For a drug hunter looking at it as a starting point, it was a minefield of liabilities:
Paralysis: Administering the drug to a living organism resulted in profound, widespread muscle paralysis and cardiovascular collapse.
Severe Cytotoxicity: It breaks down into toxic byproducts when exposed to blue light (phototoxicity), making it dangerous to cells.
Abysmal Solubility: It precipitates out of solution easily, making it virtually impossible to formulate into a pill that a human body could absorb cleanly.
Cross-Reactivity: It lacks the safety margins needed to keep from interfering with non-muscle cellular processes.
For these reasons, the biotech industry viewed skeletal myosin inhibition as a toxic mechanism that would actively rob muscular dystrophy patients of the precious little strength they had left. The industry consensus was that the entire chemical class of myosin inhibitors was inherently un-druggable for systemic human diseases. Russell bet his new company on the belief that modern computational chemistry and high-throughput biomechanical screening could completely rewrite this chemical scaffold from scratch. Russell and his team at Edgewise had to accomplish a staggering feat of molecular engineering. They used blebbistatin’s known binding interactions with the myosin head to design a drug, sevasemten (EDG-5506), that inverted the historic paradigm. Instead of shutting down contraction, sevasemten was optimized in preclinical models to spare slow-twitch postural muscles entirely and modulate the peak force of fast-twitch (Type II) fibers by an estimated 10% to 15%. This was observed to protect dystrophin-deficient cell membranes from stress-induced rupture in preclinical models, while leaving >85% of the muscle’s functional capacity completely intact in these models, thereby preserving basic strength while clipping the top-end destructive peak forces.
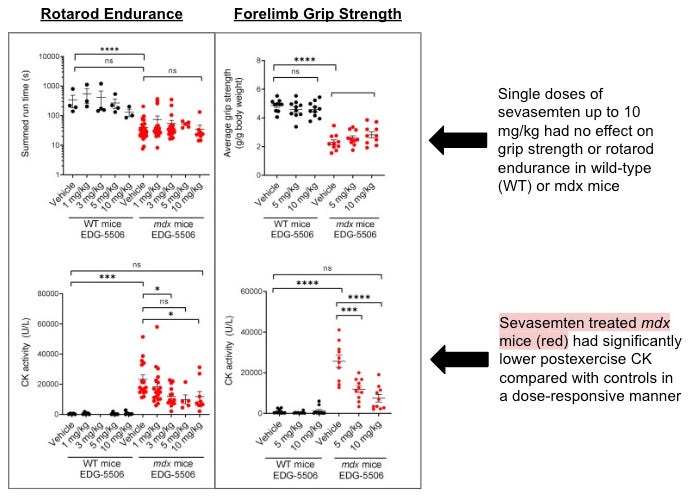
To demonstrate that their approach could have a workable therapeutic window, Edgewise evaluated sevasemten in rigorous in vivo challenge models, including the mdx mouse and the sapje zebrafish. Preclinical subjects were subjected to downstream downhill running exercises, a high-stress eccentric contraction protocol designed to rapidly degrade dystrophic muscle. Untreated or non-selectively inhibited models showed widespread sarcolemma (membrane) tearing, massive calcium influx, and profound physical exhaustion. Animals treated with sevasemten demonstrated a significant reduction in contraction-induced injury within these studies. Crucially, their overall grip strength, exercise capacity, and voluntary ambulation remained relatively unimpaired (see the graphs below).
In December 2020, Edgewise capitalized on its preclinical progress and a highly favorable biotech market by closing a $95 million Series C led by Viking Global Investors. The closing of the Series C coincided with sevasemten entering the clinic. The company initiated its Phase 1 randomized, placebo-controlled, double-blind, Single and Multiple Ascending Dose (SAD/MAD) trial (NCT04585464). The study was designed to evaluate safety, tolerability, and pharmacokinetics first in healthy adult volunteers, followed immediately by adults with Becker muscular dystrophy.
Beyond clinical execution, the $95 million injection gave Edgewise immense strategic runway. It ensured that when the company eventually pursued its IPO, it did so from a position of financial strength. On March 26, 2021, Edgewise priced its Initial Public Offering (IPO) on the Nasdaq Global Select Market. The company issued 11 million shares, raising $176 million in gross proceeds. This public capital injection gave Edgewise a massive, multi-year cash runway. It insulated the company from the broader biotech market contraction that occurred later in 2022, allowing management to fund parallel clinical portfolios without requiring immediate, dilutive follow-on financing.
With its balance sheet fortified, Edgewise focused on translating its preclinical mechanical thesis into human clinical validation, specifically targeting Becker Muscular Dystrophy (BMD). Initiated at the end of 2021, the Phase 1b ARCH study (NCT05160415) was an open-label, single-center Phase 1b follow-on evaluation tracking adult males with BMD. The goal of the study was to explore whether daily oral dosing of sevasemten safely and consistently protected against contraction-induced muscle injury over an extended timeline. On October 13, 2022, the company announced positive 6-month interim results showing that Creatine Kinase (CK) and Fast Skeletal Muscle Troponin I (TNNI2) were reduced by an average of 39% and 75%, respectively. They formally presented the data the next morning, October 14, 2022, during an Edgewise-sponsored symposium at the World Muscle Society (WMS) Congress.
Building on early ARCH data, Edgewise scaled operations internationally by launching the Phase 2 CANYON trial (NCT05291091) in 2022 to assess safety, pharmacokinetics, and functional endpoints in a larger cohort of adults and adolescents with BMD. As the CANYON trial met its early biomarker objectives, the FDA’s engagement helped shape the next phase. Although the FDA declined to review an early, accelerated approval application based strictly on initial short-term CANYON biomarker readouts, the data was robust enough to justify a larger registrational effort. Edgewise expanded the program into GRAND CANYON, a global, randomized, placebo-controlled pivotal Phase 3 cohort within the same clinical infrastructure, designed to serve as the primary vehicle for full regulatory approval. Concurrently, the company expanded the evaluation of sevasemten into Duchenne Muscular Dystrophy (DMD), initiating Phase 2 safety and biomarker cohorts to address the more severe, rapidly progressing pediatric phenotype.
While the biotech industry viewed Edgewise primarily as a skeletal-neuromuscular company, Alan Russell’s team used this period to quietly apply their sarcomere-modulation platform to cardiac muscle biology. This effort yielded EDG-7500, an entirely distinct asset. Hypertrophic Cardiomyopathy (HCM) and related forms of diastolic dysfunction arise from genetic abnormalities that cause the heart muscle to over-contract and fail to relax, restricting ventricular filling. EDG-7500 was engineered as a highly selective, next-generation cardiac sarcomere modulator. It acts as an allosteric cardiac myosin inhibitor, designed to ease hypercontractility and improve the relaxation dynamics of the left ventricle during diastole, without lowering overall systemic ejection fractions. In late 2023 and early 2024, Edgewise advanced EDG-7500 into human testing via the CIRRUS-HCM clinical program.
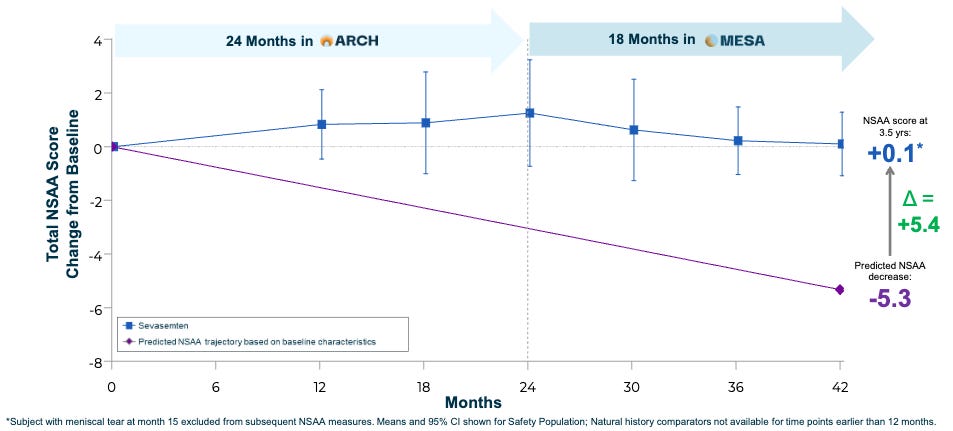
Entering 2025, the primary objective for Edgewise was to demonstrate that the biomarker reductions seen in early trials would translate into durable, multi-year physical preservation for patients with Becker Muscular Dystrophy (BMD). At the 2026 Muscular Dystrophy Association (MDA) Clinical & Scientific Conference, Edgewise presented highly anticipated data from its MESA open-label extension study. The trial tracked BMD patients on sevasemten for up to 3.5 years of continuous follow-up, demonstrating sustained functional stabilization. While a typical BMD patient experiences a predictable, progressive decline in functional mobility over 3.5 years, the sevasemten cohort maintained robust North Star Ambulatory Assessment (NSAA) scores (see graph below). Parallel to the MESA extension, Edgewise completed enrollment for its global, randomized, placebo-controlled GRAND CANYON Phase 3 trial, positioning the molecule for a planned top-line data readout in late 2026.
Three months later, Servier agreed to acquire Edgewise’s entire muscular dystrophy business, centered around sevasemten (including the active BMD and DMD programs).
Muscle Memory
But, what is Becker Muscular Dystrophy (BMD), and what shaped our understanding of this condition? Until the mid-20th century, progressive, X-linked muscle wasting in young boys was viewed almost exclusively through the lens of Duchenne Muscular Dystrophy (DMD), which had been thoroughly documented by French neurologist Guillaume-Benjamin-Amand Duchenne in the 1860s. DMD was notoriously severe, uniformly leading to a loss of ambulation in early adolescence and death in early adulthood.
That changed when, in 1955, German neurologist and geneticist Dr. Peter Emil Becker published observations of a “new type of X-chromosomal muscular dystrophy.” Dr. Becker identified families where males exhibited a nearly identical pattern of proximal muscle weakness (starting in the hips, pelvis, and thighs) but with a vastly more prolonged, variable, and milder clinical course. Unlike Duchenne patients, many of Dr. Becker’s patients retained the ability to walk well into adulthood and lived normal lifespans. For decades, this milder phenotype was clinically tracked as a distinct entity known as Becker’s Muscular Dystrophy (BMD).
For thirty years after Dr. Becker’s description, the underlying biochemical cause of both Duchenne and Becker variants remained entirely unknown. The paradigm shifted radically in the late 1980s with the advent of modern genomics. Armed with funding from organizations like the Muscular Dystrophy Association (MDA), researchers successfully cloned the DMD gene on the X chromosome, the largest known protein-coding gene in the human genome. The protein encoded by this massive gene was identified and named dystrophin. Scientists quickly realized that DMD and BMD were not separate diseases, but rather different points on the same genetic spectrum, collectively termed dystrophinopathies.
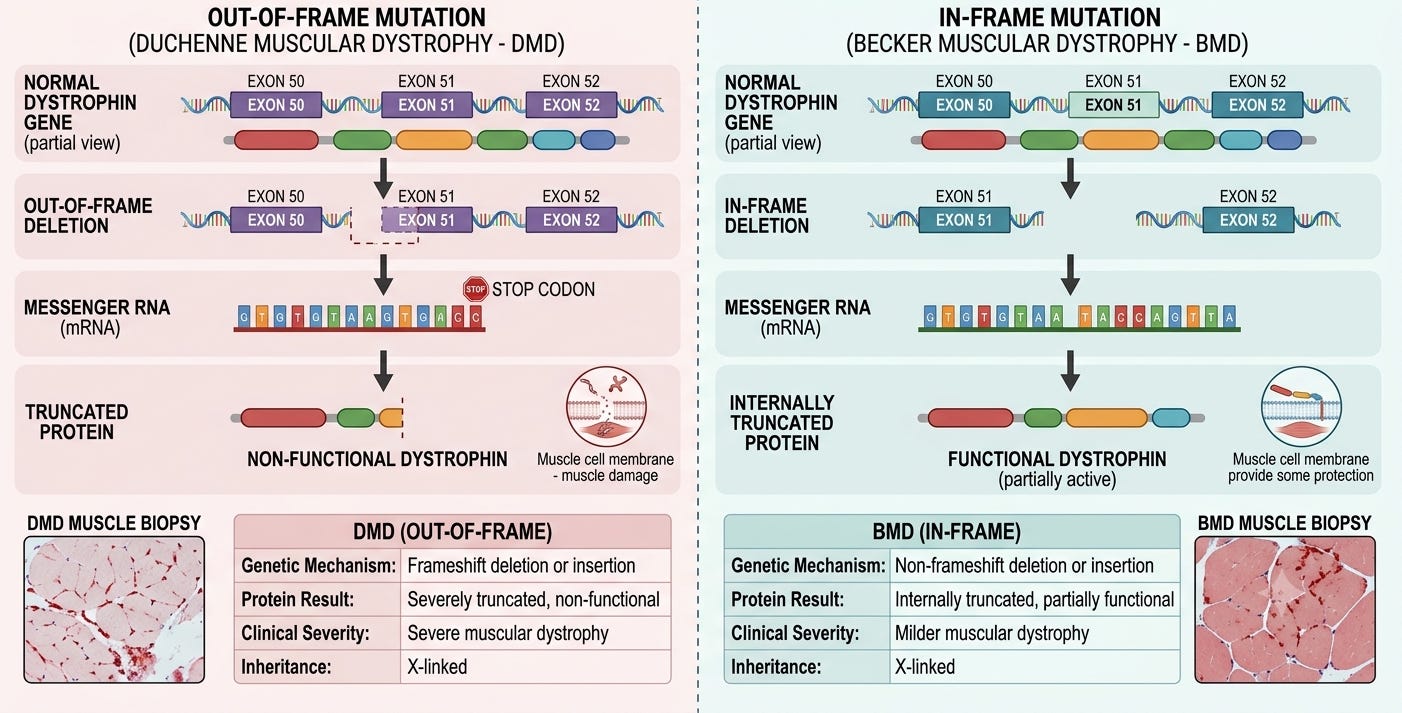
The critical historical insight came down to the biological structure of the mutation. In Duchenne patients, mutations are typically out-of-frame, completely disrupting the cell’s ability to read the genetic recipe. This results in virtually zero functional dystrophin protein. In Becker patients, mutations are typically in-frame. The cell skips over specific amino acids but manages to stitch the rest back together. This produces a shortened, partially functional version of dystrophin. It cannot anchor the muscle cell perfectly, but it provides enough structural integrity to significantly slow down muscle degeneration.
With the molecular architecture defined, the late 20th and early 21st centuries focused on establishing standards of care and testing targeted genetic therapies. Multi-center natural history studies confirmed that while steroids (like prednisone) could delay functional decline by dampening chronic muscle inflammation, they introduced heavy metabolic side effects and did not fix the underlying structural flaw. Since Becker patients proved that a shortened dystrophin protein could support a relatively normal lifestyle, the biopharma industry poured billions into developing exon-skipping antisense oligonucleotides (ASOs). The goal was to artificially convert a severe Duchenne “out-of-frame” mutation into a milder, Becker-like “in-frame” profile. Paradoxically, while Becker biology served as inspiration for saving Duchenne patients, actual BMD patients were largely excluded from advanced clinical development pipelines for decades, left with few therapeutic options beyond supportive physical therapy and routine cardiac monitoring for dilated cardiomyopathy.
Historically, treating BMD meant waiting for genetic tools to advance. However, the modern clinical era has shifted toward treating the disease as a mechanical engineering problem. In the 2020s, advanced biophysical research consolidated the understanding that without a full complement of dystrophin, everyday fast-twitch (Type II) muscle contractions generate immense physical force that tears the vulnerable muscle membrane (sarcolemma), leading to chronic enzyme leakage (like Creatine Kinase) and muscle death. This insight led to the creation of novel small-molecule therapies designed not to rewrite the gene, but to modify muscle mechanics. The development of molecules like sevasemten (EDG-5506), an allosteric fast-skeletal myosin inhibitor, is being evaluated to determine if subtly dampening peak contraction forces can protect Becker muscle fibers from contraction-induced damage.
Conclusion
Servier’s acquisition of Edgewise’s muscular dystrophy pipeline highlights a maturing trend in biotech: the monetization of robust, long-term Phase 2 data to fund earlier-stage platform depth. The 3.5-year MESA extension data may have provided the compelling clinical signal Servier needed to make a $2.65 billion bet. For Edgewise, the $1.55 billion upfront cash windfall significantly extends the company’s projected operational runway. All eyes now pivot to their cardiac sarcomere modulators, EDG-7500 and EDG-15400. Armed with substantial non-dilutive capital, Edgewise is well-positioned to advance its cardiovascular pipeline.
To contact us, please send us an email at biotechreadout@gmail.com
Disclaimers
Investigational Status Disclaimer
The therapeutic candidates discussed in this newsletter are currently in clinical development and have not been approved for commercial sale by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), or other global regulatory authorities. Their safety and efficacy have not been established. References to pipeline products and ongoing clinical trials involve significant risks and uncertainties. Statements regarding the potential safety, potency, or efficacy of investigational drugs reflect current hypotheses and are not a guarantee of future performance or regulatory clearance. The outcome of clinical trials is inherently unpredictable, and clinical results from earlier stages may not be predictive of results in later, larger-scale trials.
No Medical Advice Disclaimer
This newsletter is for informational and educational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this publication.
No Patient-Provider Relationship Disclaimer
The information provided in this newsletter is for educational and analytical purposes only. Receipt of this information, or any interaction with this content, does not create a physician-patient, pharmacist-patient, or any other professional-provider relationship between you and the authors or publishers. This newsletter should not be used as a substitute for a personal consultation with a qualified healthcare professional.
Forward-Looking Statements Disclaimer
This newsletter contains “forward-looking statements” regarding future events, including clinical trial timing, regulatory milestones, and projected market performance. These statements are based on current expectations and assumptions that are subject to significant risks and uncertainties. Actual results may differ materially from those expressed or implied. We undertake no obligation to update these statements as a result of new information or future developments.
Third-Party Links & Content Disclaimer
This newsletter contains links to third-party websites, including clinical trial registries and corporate presentations. Biotech Readout does not endorse, guarantee, or assume responsibility for the accuracy or reliability of any information offered by third-party providers.
Errors and Omissions Disclaimer
While we strive for technical accuracy, the information in this newsletter is provided on an “as is” basis with no guarantees of completeness, accuracy, or timeliness. Biotech Readout assumes no liability for any errors or omissions in the content of this publication.
Non-Endorsement Disclaimer
Any reference to specific commercial products, processes, or services by trade name, trademark, or manufacturer does not constitute or imply an endorsement or recommendation by the author. All trademarks are the property of their respective owners.
No Investment Advice Disclaimer
This newsletter is for informational purposes only and does not constitute financial, investment, or legal advice. The author is not a registered investment advisor. You should consult with a professional financial advisor before making any investment decisions. The biotechnology sector is highly volatile; past performance is not indicative of future results.
Conflict of Interest Disclaimer
The author of this newsletter maintains a position of independence. At the time of publication, the author holds no direct financial interest, equity, or options in any of the companies mentioned in this report. No compensation has been received from any third party to feature or analyze specific therapeutic candidates or corporate entities.