
Ipsen to Acquire Memo
Neutralizing the viral ghosts that haunt kidney transplant patients

Disclaimer: This newsletter is for educational and informational purposes only and does not constitute medical, investment, or financial advice, nor does it establish a provider-patient relationship. Content may include forward-looking statements and discussions of investigational therapeutic candidates that are not FDA/EMA approved; their safety and efficacy remain unestablished and clinical outcomes are unpredictable. While we strive for accuracy, all information is provided as is without guarantees. As of the date of publication, the author holds no direct equity positions in the specific companies mentioned in this issue nor receives third-party compensation for this coverage. Please find a complete version of our disclaimers at the bottom of this article and on our About page.

Introduction
On July 1, 2026, Ipsen announced a definitive agreement to acquire Memo Therapeutics AG for €200 million (about $228 million USD) upfront at closing and up to a total of €700 million (about $797 million USD) contingent upon the achievement of specified development, regulatory approval and sales-based milestones (Ipsen press release, Memo press release). This acquisition centers on potravitug, an investigational first-in-class BK polyomavirus (BKV) monoclonal antibody that is currently being evaluated for the treatment of active BK polyomavirus associated nephropathy (BKVAN) and the prevention of graft loss or transplant failure in kidney transplant patients.
In this article, we dive into the history of BK polyomavirus (BKV), uncover the foundational discoveries that enabled Memo Therapeutics’ potravitug, and relive the company’s fascinating backstory.
Hidden Plague
BK polyomavirus (BKV) is a small, double-stranded DNA virus belonging to the Polyomaviridae family that is highly ubiquitous in the human population, with up to 90% of adults worldwide maintaining a lifelong, asymptomatic latent infection within the epithelial cells of the kidney and urinary tract. While the virus is benign in individuals with intact immune systems, it presents a severe clinical threat to kidney transplant recipients. For context, kidney transplant patients must take a cocktail of immune suppressing medicines after a transplant so that the donor organ can engraft and start working. However, that cocktail makes the patient functionally immunocompromised, with a diminished capacity to defend against infectious diseases. When host immunity is suppressed, BKV can reactivate and undergo unchecked lytic replication, leading to severe complications such as BK virus-associated nephropathy (BKVAN). BKVAN can cause premature kidney allograft failure, or hemorrhagic cystitis, characterized by painful bladder inflammation and bleeding.
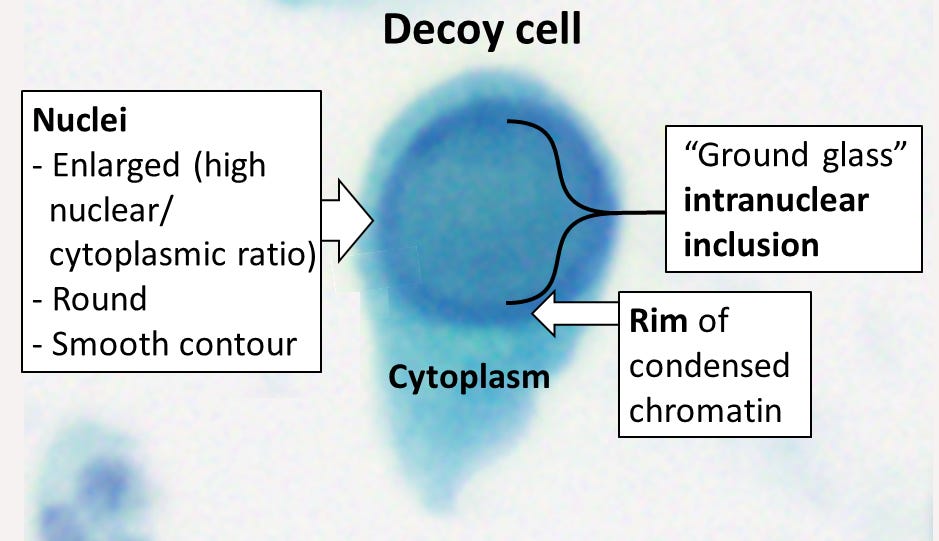
But, how did we discover BKV if it’s invisible to most people? This story of its discovery is a journey from an accidental virological discovery to an emerging clinical challenge. The virus was first isolated in 1970 at the Virus Research Laboratory in London, England. A virologist named Dr. Sylvia Gardner was investigating the epidemiology of a different virus, cytomegalovirus (CMV). While examining the urine of a 39-year-old Sudanese kidney transplant recipient who had developed a severe ureteric stricture (narrowing of the ureter), Dr. Gardner noted numerous cells containing prominent viral inclusions. Using electron microscopy, Dr. Anne Field identified viral particles that structurally resembled papillomaviruses. Once successfully cultured and confirmed as a distinct, novel agent, the virus was named “BK” after the initials of that first patient. The original viral isolate is still referred to as the Gardner strain. The discovery was formally published in a landmark 1971 issue of The Lancet, in a back-to-back sequence with the discovery of the closely related JC polyomavirus (JCV).
Following the isolation of BKV, extensive serological and epidemiological studies revealed a striking paradox: while the virus was discovered in a severely ill transplant patient, it was actually ubiquitous in the general population. Researchers discovered that primary BKV infection typically occurs in early childhood (often by age 4 or 5), spreading asymptomatically via respiratory or fecal-oral routes. By adulthood, 80% to 90% of the global population is seropositive. Investigators realized that after the primary childhood exposure, the virus establishes a lifelong, silent residency (latency) within the renal tubular epithelial cells and the urothelium of the urinary tract. Since it remains completely benign and asymptomatic in healthy individuals, BKV was largely categorized as an opportunistic pathogen of low clinical priority throughout the 1970s and 1980s.
The clinical significance of BKV changed dramatically in the late 20th century, driven by a major evolution in transplant medicine: the introduction of highly potent, next-generation immunosuppressive drugs (such as tacrolimus and mycophenolate mofetil) in the mid-1990s. In 1993, at the University of Pittsburgh, clinicians documented the first definitive, biopsy-proven case of BK virus-associated nephropathy (BKVAN), then termed polyomavirus interstitial nephritis, in a kidney transplant recipient presenting with unexplained graft dysfunction. As these potent triple-drug immunosuppressive regimens became the global standard of care to prevent organ rejection, rates of BKV reactivation skyrocketed. Unchecked viral replication leads to a vicious cascade: viruria (shedding in urine), progressing to viremia (virus entering the bloodstream), and ultimately resulting in BKVAN, a leading cause of premature kidney allograft loss. Concurrently, BKV emerged as a primary culprit behind hemorrhagic cystitis (characterized by severe, painful bladder inflammation and bleeding) in bone marrow and stem cell transplant recipients.
Today, BKV remains a factor in transplant success. Since there are still no universally approved, highly effective antiviral medications specifically targeting BKV, clinical management historically relies on a delicate balancing act: reducing a patient’s immunosuppression to allow their own immune system to clear the virus, which simultaneously spikes the risk of acute organ rejection.
Secrets in the Serum
For decades after the discovery of the virus in 1971, the role of antibodies in controlling BKV was highly debated. Researchers knew that 80% to 90% of adults were seropositive for BK virus, yet immunosuppressed patients still suffered from severe viral reactivation leading to BK virus-associated nephropathy (BKVAN). Early serology relied on hemagglutination inhibition (HI) assays, which lacked the sensitivity to distinguish true virus neutralization from broad cross-reactive binding. Since patients with high antibody titers still developed active viremia, the initial medical consensus was that humoral immunity was largely ineffective, and that viral control depended almost entirely on cell-mediated (T-cell) immunity.
The modern understanding of BKV neutralizing antibodies was unlocked by a critical technological breakthrough: the development of BK polyomavirus pseudoviruses (BK-PsVs), pioneered heavily by researchers like Diana Pastrana and Christopher Buck at the National Institutes of Health (NIH). By engineering pseudoviruses that packaged a reporter gene (such as green fluorescent protein or luciferase) inside recombinant viral capsid proteins (VP1, VP2, VP3), scientists could finally measure actual in vitro neutralization in cell culture. Utilizing these pseudovirus systems, researchers demonstrated that the four major genomic variants of BKV (Genotypes I-IV) behaved as completely distinct serotypes. An antibody that neutralized Genotype I would often fail to neutralize Genotype IV, explaining why a patient could have high total antibody titers but still be susceptible to a different, donor-derived strain of the virus.
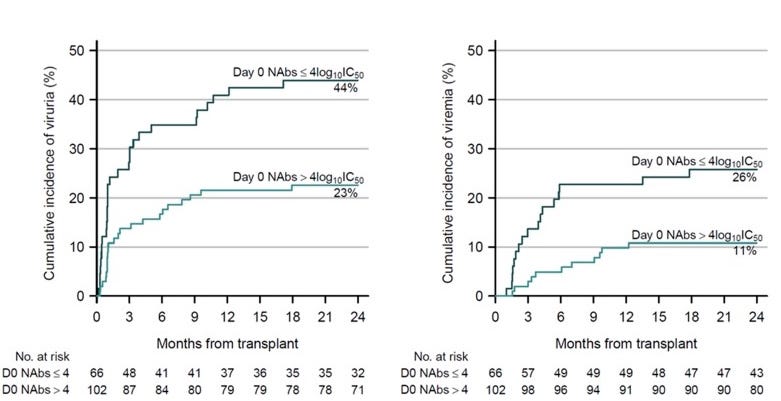
Equipped with functional neutralization assays, clinical cohorts were closely monitored. The landmark 2018 study published in the Journal of the American Society of Nephrology (JASN) was conducted by a highly collaborative, multidisciplinary team of clinical and research experts based out of Strasbourg University Hospital (Hôpitaux Universitaires de Strasbourg) and the University of Strasbourg. It demonstrated that kidney transplant recipients who possessed high pre-transplant neutralizing antibody titers specifically matched to their donor’s BKV serotype were profoundly protected against post-transplant viruria (virus in the urine) and viremia (virus in the blood). A neutralizing antibody (NAb) titer <4 log10 IC50 on the day of transplantation was associated with an 88% higher risk of BKV replication after transplantation (HR, 1.88; 95% CI, 1.06 to 3.45; P=0.03).
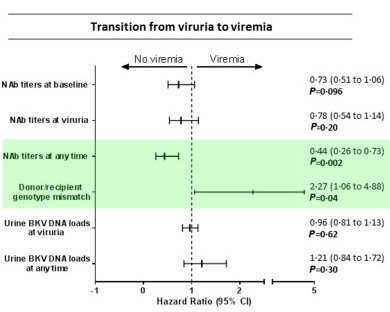
Why did patients with neutralizing antibodies above the threshold still develop BKV infection? About 17% of patients with viruria lacked neutralizing antibodies against the specific strains of BKV that they contracted, a mismatch that allowed infection to slip through the cracks. While patients with neutralizing antibody titers during the observation period came with a 56% lower risk of transitioning from viruria (local infestation) to viremia (more global infestation), antibody mismatch with the replicating strain nevertheless resulted in a 2.3-fold increased risk of viremia. It’s not enough to simply have neutralizing antibodies. They have to hit the relevant strain in order to effectively reduce the risk of infection.
Making Medicines
With clinical pathophysiology established, the race began to isolate potent, pan-serotype human monoclonal antibodies capable of blocking all four genotypes without allowing for easy mutational escape.
Researchers at Amplyx Pharmaceuticals successfully isolated P8D11, a human-derived antibody with picomolar affinity that targeted a highly conserved structural epitope on the major capsid protein VP1. P8D11 blocked the viral attachment mechanism to host sialic acid receptors. This antibody was subsequently humanized and advanced into clinical development as MAU868. When Pfizer acquired Amplyx for an undisclosed amount in 2021 to secure its anti-fungal portfolio, the BKV program sat outside Pfizer’s core therapeutic focus. In late 2021, Vera Therapeutics acquired MAU868 from Amplyx/Pfizer for a rather paltry $5 million upfront plus up to $7 million upon reaching certain regulatory milestones. For Vera, a biotechnology company heavily anchored in serious kidney-related diseases, MAU868 was a good fit in its pipeline.
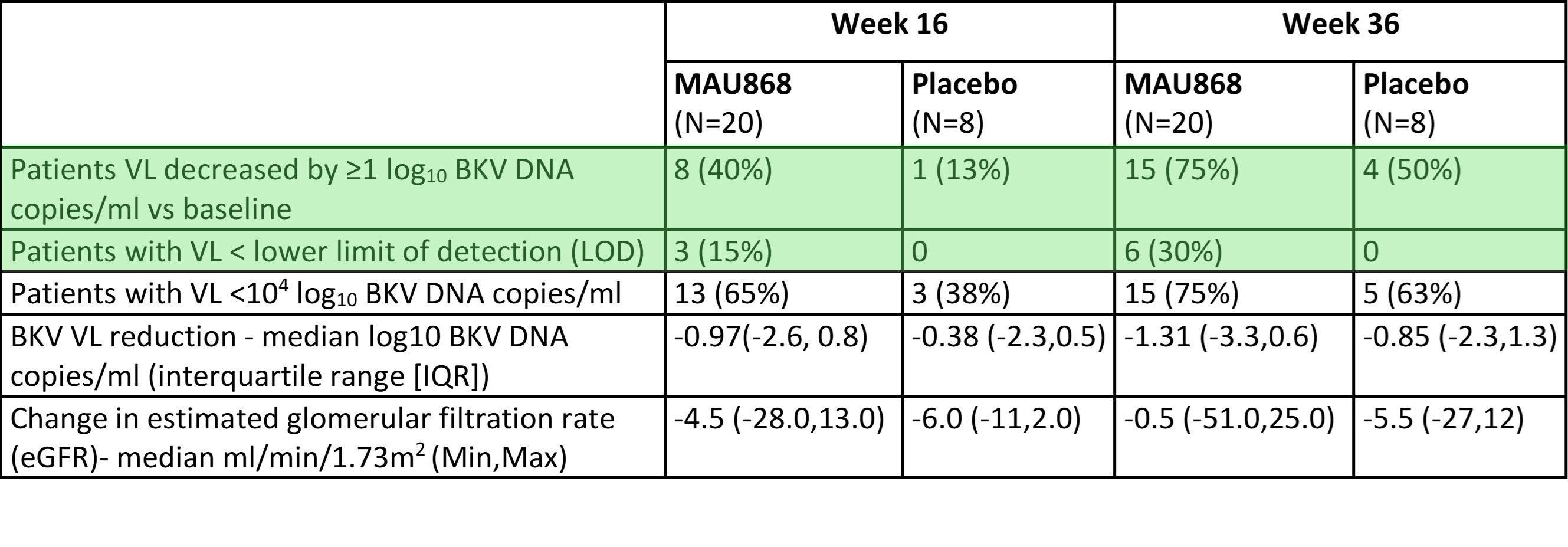
Vera took over and presented data from a randomized, double-blind, placebo-controlled Phase 2 study evaluating MAU868 in adult kidney transplant recipients who had developed active BK viremia within one year post-transplant. Participants were randomized (2:1) to receive four intravenous doses every 28 days across two distinct treatment cohorts or a matching placebo. Vera first presented the interim 12-week topline data for MAU868 at the American Transplant Congress (ATC) on June 4, 2022, in a late-breaking oral presentation. Following that initial look, Vera shared the final, full 36-week results later that year at the American Society of Nephrology (ASN) Kidney Week annual meeting in November 2022. By Week 36, more MAU868-treated patients achieved a ≥1 log10 reduction in plasma viral load (75% versus 50% for placebo), and reduced viral loads below the lower limit of quantification (30% versus 0% for placebo), showing that a passive antibody therapy can effectively manage post-transplant BK virus replication without requiring hazardous adjustments to a patient’s core immunosuppressive regimen.
Despite this early success, Vera has shifted nearly all of its near-term corporate energy, funding, and public focus toward their lead asset, atacicept, whose PDUFA target action date for IgA Nephropathy (IgAN) is less than a week away from this article’s time of publication (July 7, 2026). The molecule appears to be in limbo, neither discontinued nor advanced into the larger Phase 2b/3 that Vera telegraphed back in 2022.
However, progress in the field didn’t stop with MAU868. Memo Therapeutics was founded in 2012 as a spin-off from the Swiss Federal Institute of Technology (ETH Zurich). Headquartered in the biotech hub of Schlieren/Zurich, Switzerland, the company was co-founded by Dr. Christoph Esslinger (who long served as Chief Scientific Officer) and a team of molecular biologists. In 2018, Memo raised their Series A, bringing in Swiss-based Verve Ventures, which anchored the company’s early expansion. The company was built entirely around a singular technological breakthrough: the DROPZYLLA platform. Rather than engineering synthetic antibodies in a lab or using humanized mice, DROPZYLLA was designed as an “antibody repertoire copying engine.” It used single-cell microfluidics to isolate individual memory B cells from rare human donors, specifically elite neutralizers, or rare patients who had naturally beaten severe viral infections or cancers. This could effectively capture the best blueprints of the human immune system.
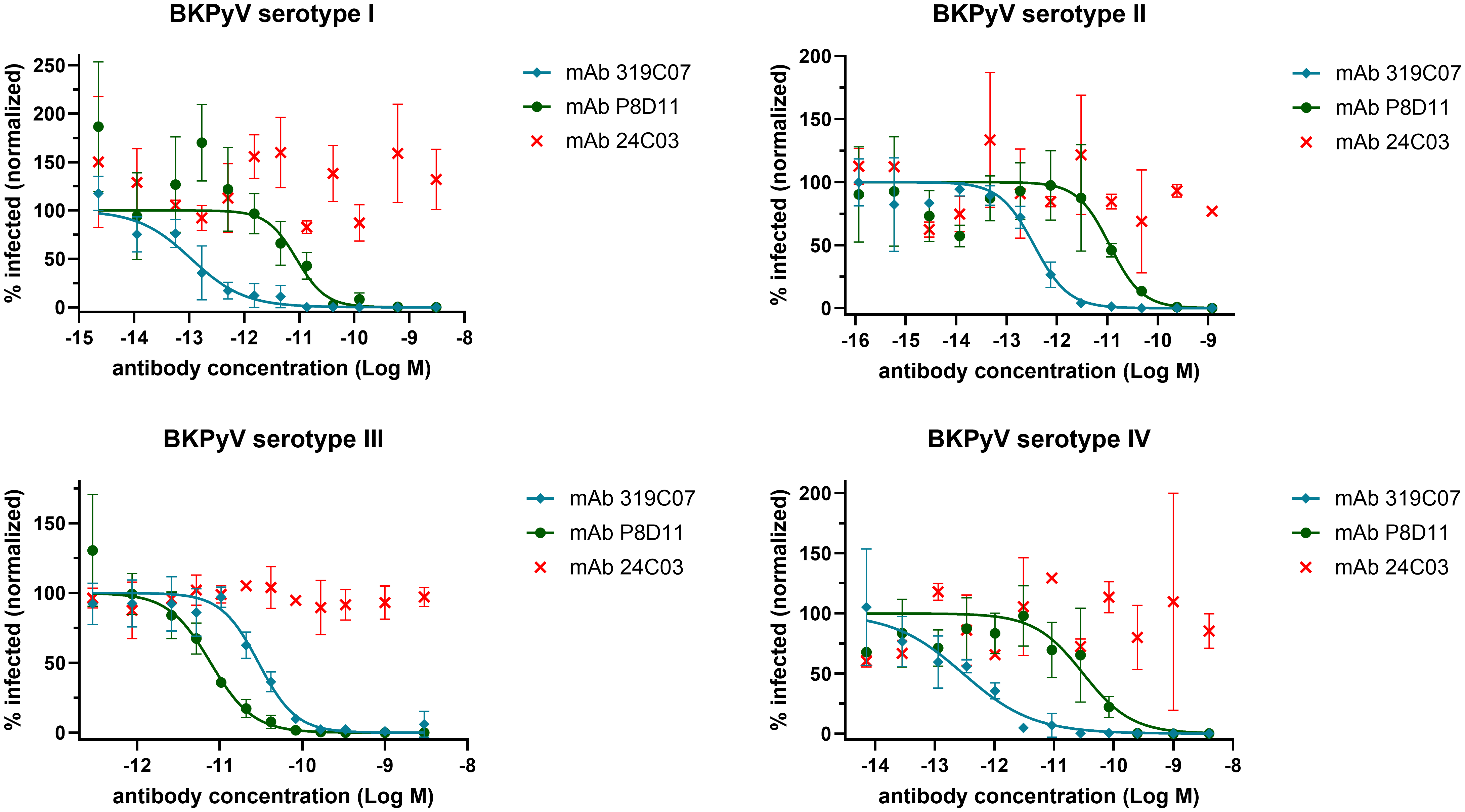
In 2021, they pointed their DROPZYLLA platform not at BKV, but at COVID-19. Amid the global pandemic, Memo closed a CHF 13.8 million Series B round led by Swisscanto and rapidly validated its platform by isolating a highly potent, fully human neutralizing antibody (MTX-COVAB) from convalescent COVID-19 donors in just three weeks. Preventative vaccines beat them to the punch, and COVID-19 dropped off of the priority list. However, they had been working on a second program. Scientists at Memo had begun screening the B-cell repertoires of elite neutralizers of BKV, rare transplant patients who rapidly cleared massive BK viral loads on their own. They once again leveraged their DROPZYLLA platform to clone the paired antibody genes from elite neutralizers of BKV into mammalian expression vectors, creating a recombinant library of their immune responses. They then ran high-throughput functional screens using BKV pseudoviruses to identify candidates that blocked cell entry. Out of millions of candidates, mAb 319C07 (potravitug) emerged as the winner. It exhibited exceptional picomolar binding affinity to a highly conserved, conformationally complex structural epitope on the VP1 capsid pentamer. Since this specific epitope is indispensable for the virus to attach to host sialic acid receptors, potravitug exerts a structural blockade that prevents cell-to-cell viral spread across all four major BKV serotypes (see graph below).
Armed with this ultra-potent molecule, Memo raised a $25 million Series C round in late 2023 led by Pureos Bioventures. In May 2024, they secured a CHF 20 million Series C extension (bringing the total round to CHF 45 million), adding investors like Ysios Capital and Kurma Partners. This capital was deployed to evaluate potravitug in the Phase 2 SAFE KIDNEY II trial (NCT05769582), the largest randomized, double-blind, placebo-controlled trial ever conducted for the treatment of BKV-associated nephropathy (BKVAN). The study enrolled 95 kidney transplant recipients across 22 sites in the U.S. who had active, high-load BKV DNAemia (≥ 10,000 IU/mL). Patients received four intravenous infusions of either potravitug (500 mg or 1000 mg) or a placebo, spaced 4 weeks apart, on top of standard-of-care immunosuppression adjustments. Initial analyses from the study were first shared at the 63rd European Renal Association (ERA) Congress in early June 2026, followed immediately by the presentation of the complete, long-term 38-week dataset at the American Transplant Congress (ATC) on June 23, 2026. By week 38, 24.4% of potravitug-treated patients achieved plasma BKV-DNAemia below the lower limit of quantification compared to 13.0% in the placebo cohort, with a ≥2 log10 reduction in viral load observed in 40.3% versus 24.7% of patients, respectively. Crucially, protocolized kidney biopsies at week 20 revealed that active, biopsy-proven BKVAN declined from 51.2% to 31.6% in the treatment arm while remaining completely unchanged in the placebo group, all while demonstrating a generally well-tolerated safety profile with no treatment-related serious adverse events.
A few weeks lated on July 1, 2026, the global biopharmaceutical giant Ipsen announced a definitive agreement to acquire Memo Therapeutics, securing potravitug for its expanding rare disease portfolio. To separate the drug from the platform in the transaction, a condition of the acquisition required a corporate split. While Ipsen absorbed the potravitug program to push it into global Phase 2/3 trials, Memo’s original discovery foundations are set to be spun off into a newly incorporated entity named Memorises Bio that encompasses:
The proprietary DROPZYLLA platform
An ongoing recombinant polyclonal IgG collaboration with CSL
Its early-stage oncology pipeline
Memorises Bio is to remain held by Memo’s original shareholders and will continue finding the next generation of human antibodies.
Conclusion
Memo Therapeutics’ development effort is a text-book validation of reverse-translational medicine. By hunting for answers within the immune systems of rare elite neutralizers, scientists bypassed traditional lab-bench guesswork to uncover a neutralizing antibody optimized by nature. In acquiring potravitug, Ipsen secures a pan-serotype weapon against a historically hard to treat post-transplant threat. As potravitug marches toward global Phase 2/3 trials under Ipsen’s rare disease banner, the legacy of the DROPZYLLA engine lives on. The birth of Memorises Bio ensures that the hunt for the next generation of natural human antibodies continues. If pivotal trials succeed and the medicine passes through regulatory review, it could someday allow clinicians to treat active BKVAN without forcing a hazardous compromise on a patient’s core immunosuppressive safety net.
Love biotech? Check out Biotech Readout’s full content library, or navigate directly to a segment that interests you:
Frontiers in Medicine: Exploring the frontiers of our understanding and treatments for disease.
Medical History: Recovering forgotten relics in the history of medicine.
Acquisitions: Exploring the innovation behind acquired companies.
Weekly Readout: A digest of new clinical data from the past week.
To contact us, please send us an email at biotechreadout@gmail.com
Disclaimers
Investigational Status Disclaimer
The therapeutic candidates discussed in this newsletter are currently in clinical development and have not been approved for commercial sale by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), or other global regulatory authorities. Their safety and efficacy have not been established. References to pipeline products and ongoing clinical trials involve significant risks and uncertainties. Statements regarding the potential safety, potency, or efficacy of investigational drugs reflect current hypotheses and are not a guarantee of future performance or regulatory clearance. The outcome of clinical trials is inherently unpredictable, and clinical results from earlier stages may not be predictive of results in later, larger-scale trials.
No Medical Advice Disclaimer
This newsletter is for informational and educational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this publication.
No Patient-Provider Relationship Disclaimer
The information provided in this newsletter is for educational and analytical purposes only. Receipt of this information, or any interaction with this content, does not create a physician-patient, pharmacist-patient, or any other professional-provider relationship between you and the authors or publishers. This newsletter should not be used as a substitute for a personal consultation with a qualified healthcare professional.
Forward-Looking Statements Disclaimer
This newsletter contains “forward-looking statements” regarding future events, including clinical trial timing, regulatory milestones, and projected market performance. These statements are based on current expectations and assumptions that are subject to significant risks and uncertainties. Actual results may differ materially from those expressed or implied. We undertake no obligation to update these statements as a result of new information or future developments.
Third-Party Links & Content Disclaimer
This newsletter contains links to third-party websites, including clinical trial registries and corporate presentations. Biotech Readout does not endorse, guarantee, or assume responsibility for the accuracy or reliability of any information offered by third-party providers.
Errors and Omissions Disclaimer
While we strive for technical accuracy, the information in this newsletter is provided on an “as is” basis with no guarantees of completeness, accuracy, or timeliness. Biotech Readout assumes no liability for any errors or omissions in the content of this publication.
Non-Endorsement Disclaimer
Any reference to specific commercial products, processes, or services by trade name, trademark, or manufacturer does not constitute or imply an endorsement or recommendation by the author. All trademarks are the property of their respective owners.
No Investment Advice Disclaimer
This newsletter is for informational purposes only and does not constitute financial, investment, or legal advice. The author is not a registered investment advisor. You should consult with a professional financial advisor before making any investment decisions. The biotechnology sector is highly volatile; past performance is not indicative of future results.
Conflict of Interest Disclaimer
The author of this newsletter maintains a position of independence. At the time of publication, the author holds no direct financial interest, equity, or options in any of the companies mentioned in this report. No compensation has been received from any third party to feature or analyze specific therapeutic candidates or corporate entities.