
Incyte to Acquire Vega
A bold bet on novel discoveries in a rare bleeding disorder pays off

Disclaimer: This newsletter is for educational and informational purposes only and does not constitute medical, investment, or financial advice, nor does it establish a provider-patient relationship. Content may include forward-looking statements and discussions of investigational therapeutic candidates that are not FDA/EMA approved; their safety and efficacy remain unestablished and clinical outcomes are unpredictable. While we strive for accuracy, all information is provided as is without guarantees. This newsletter is independent, and the author holds no financial positions in the companies mentioned nor receives third-party compensation for this coverage. Please find a complete version of our disclaimers at the bottom of this article and on our About page.

Introduction
On June 8, 2026, Incyte announced a definitive agreement to acquire Vega Therapeutics, Inc., a wholly owned subsidiary of Star Therapeutics, LLC, for $1.25 billion in upfront payments and up to $750 million in additional payments upon the achievement of sales milestones, for total potential consideration of up to $2.0 billion subject to customary closing adjustments. This acquisition centers on VGA039, a first-in-class monoclonal antibody currently in Phase 3 trials for the treatment of von Willebrand disease (VWD).
Here, we dive into the founding of Vega Therapeutics and its TopCo (Star Therapeutics), as well as the novel biology that enabled them to buck the trend of me-too R&D and pioneer a new drug class for treating von Willebrand disease (VWD).
The Second Spoke
The story of Vega Therapeutics is a textbook modern biotechnology narrative: an elegant concept of novel biology incubated inside an innovation engine, spun out into a laser-focused entity, and ultimately acquired in a multi-billion-dollar deal. The story begins in San Francisco in 2018 with the founding of Star Therapeutics, LLC by scientist and entrepreneur Adam Rosenthal, Ph.D. Rather than operating as a traditional biotech pursuing a single molecule, Star was designed as a “hub-and-spoke” company, a corporate structure where a central parent organization (the hub) provides capital, operational infrastructure, and shared expertise to incubate and manage a portfolio of distinct, specialized subsidiary companies (the spokes). Its core philosophy was to discover best-in-class antibody therapies targeting novel biological pathways, utilizing a unique pipeline-in-a-product strategy.
While mapping out overlooked gaps in hematology, the Star team recognized a critical unmet need in bleeding disorders, specifically von Willebrand disease (VWD), the most common inherited bleeding disorder in the world. The existing standard of care required patients to undergo burdensome, multi-weekly intravenous (IV) infusions of clotting factor to manage or prevent debilitating bleeds. Star’s scientists discovered a way to elegantly bypass this by engineering a monoclonal antibody, VGA039, designed to target Protein S. By modulating Protein S, the antibody could effectively rebalance the body’s natural coagulation cascade and improve hemostasis. Crucially, it was engineered to be administered as a convenient, once-monthly subcutaneous injection.
In late 2022, Star officially spun out Vega Therapeutics, Inc. as a dedicated home for its bleeding disorder portfolio, backing the new entity with an initial $40 million in internal financing. This was the second company (spoke) spun out of Star Therapeutics, following the formation of Elektra in early 2022 (focused on anti-SIRP mAb ELA026 for a rare hyper-inflammatory condition called Secondary Hemophagocytic Lymphohistiocytosis). Vega operated with a lean, specialized team, sharing the broader scientific and operational infrastructure of Star. Over the next two years, Vega quietly developed VGA039. The U.S. FDA recognized the therapeutic potential of the mechanism, granting VGA039 Breakthrough Therapy, Fast Track, Orphan Drug, and Rare Pediatric Disease designations.
Star Therapeutics’ presentation of interim data for VGA039 at the 67th American Society of Hematology (ASH) Annual Meeting in December 2025 provided promising clinical efficacy signals. The presentation highlighted findings from an ongoing Phase 1/2 multi-dose study. Crucially, it included cohorts that captured patients across all major subtypes of von Willebrand disease (Type 1, Type 2, and Type 3). This is a critical regulatory and clinical differentiator, as standard-of-care options vary widely depending on the patient’s specific VWF defect. The most compelling data came from patients who transitioned to VGA039 from standard-of-care intravenous (IV) clotting factor replacement regimens (which typically require highly burdensome IV infusions multiple times per week). In this subgroup, switching to monthly subcutaneous injections of VGA039 achieved a 73-100% reduction in Annualized Bleeding Rate (ABR), suggesting that some patients achieved complete bleed freedom. Achieving up to a 100% reduction by targeting Protein S proves that bypassing the body’s natural brakes on clotting works incredibly well, regardless of the patient’s specific genetic subtype of von Willebrand disease (VWD). Armed with this data and bolstered by Star’s massive $125 million Series D financing round in September 2025, Vega pushed its lead asset into a registrational trial. In October 2025, it initiated the global VIVID-6 study, a Phase 3 pivotal trial evaluating subcutaneous VGA039 across all types of VWD.
By the spring of 2026, Vega’s Phase 3 asset had captured the attention of the broader biopharmaceutical industry. Star Therapeutics and its premier venture capital backers and began working with financial advisors to explore a public listing (IPO) for the company. However, the rapid progression of the VIVID-6 trial coincided perfectly with a strategic shift at a major pharmaceutical peer: Incyte Corporation. Incyte’s newly appointed CEO, Bill Meury, was actively hunting for a late-stage hematology asset. Vega’s asset fit the bill exactly. On June 8, 2026, the narrative reached its climax. Incyte and Star Therapeutics announced a definitive agreement for Incyte to acquire Vega Therapeutics in an all-cash equity transaction.
Following the close of the transaction (expected in the third quarter of 2026), Vega Therapeutics will fully integrate into Incyte’s commercial hematology footprint, ensuring that the global scale of a major biopharma engine powers the remaining development of VGA039. Meanwhile, Star Therapeutics will continue to operate as an independent entity in San Francisco, retaining its remaining pipeline of complement-directed antibody therapies and validating its unique corporate model of incubating, proving, and successfully spinning out high-value biotech breakthroughs.
The Courage of First-in-Class
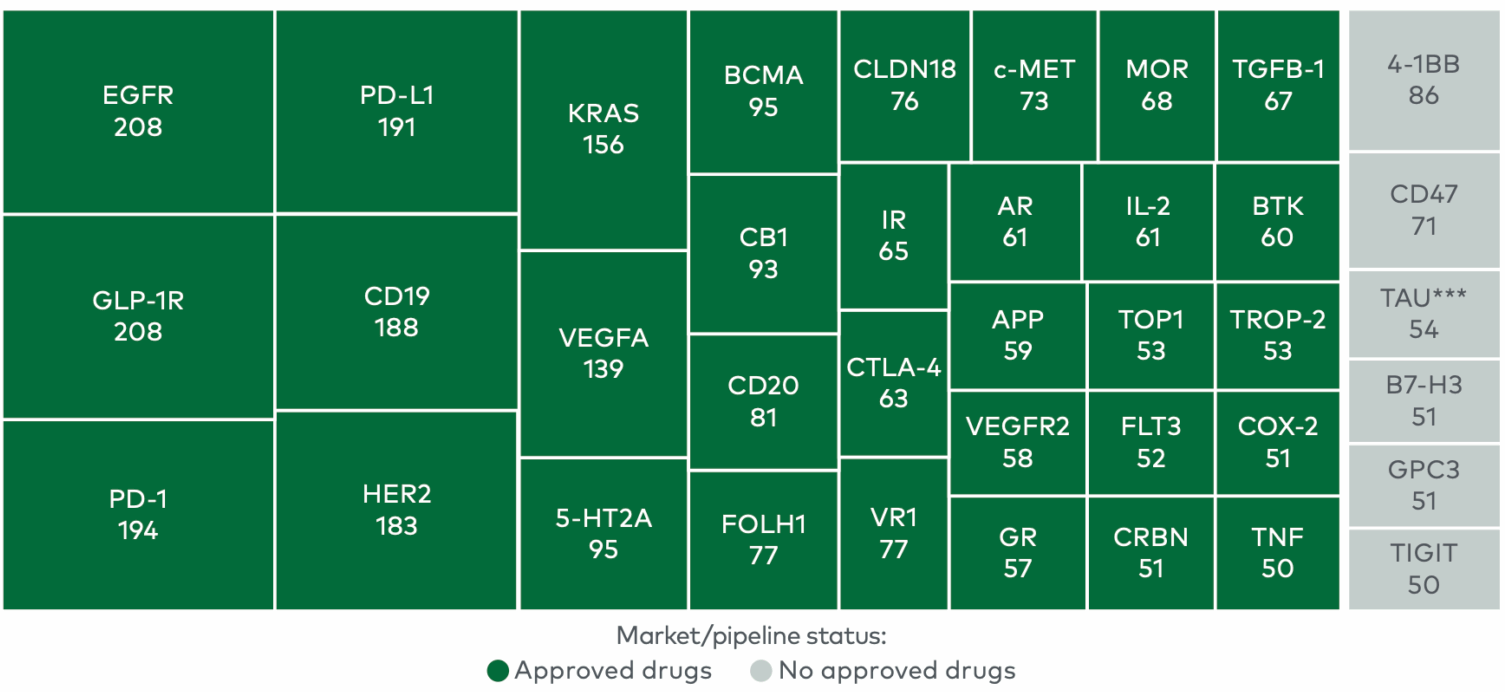
In a May 2025 article entitled Biotech Wisdom Of The Crowds: Competition And Capitalism, Bruce Booth (Partner at Atlas Venture) addresses the staggering level of “therapeutic crowding” in the biotech industry. Therapeutic crowding occurs when a massive influx of biotechnology and pharmaceutical companies simultaneously rush to develop drugs against the exact same biological target or disease indication. Driven by a herd mentality following a major scientific breakthrough or clinical validation, this intense duplication leads to a market saturated with me-too or fast-follower drugs. Notable examples include over 200 GLP-1 obesity programs and 300+ PD-1/PD-L1 cancer programs in development in early 2025.
The reason for crowding is incredibly clear. Uncovering new biology is high-risk, incredibly slow, and prone to failure, which is precisely why the industry defaults to crowding around known targets. In a separate essay published in 2017 and entitled Four Decades Of Hacking Biotech And Yet Biology Still Consumes Everything, Booth emphasizes that the primary failure mode in drug R&D is that human biology is massively complicated. We frequently pick the wrong target to interrogate, leading to massive attrition in Phase 2 trials when the hypothesis fails in humans.
Since trailblazing into unmapped biology is terrifyingly high-risk, Booth notes that capitalism naturally pushes a large portion of the industry toward “safer” fast-follower strategies. He points out that discovering and validating a brand-new biological pathway within academia is extraordinarily difficult. Translating that novel science into a structured industry setting requires drug hunters with a specific mindset who have no fear of failure, because exploring new biological frontiers means dealing with constant, iterative failure before finding a signal. When a biotech company decides to explore a completely unmapped biological mechanism, it cannot rely on off-the-shelf tools. They must build bespoke cell-based assays and find specialized contract research organizations (CROs) capable of running highly customized animal or cellular models. While global CROs are highly adept at standard, commoditized readouts, they routinely struggle with the nuanced, unscripted biology required to validate a brand-new therapeutic hypothesis.
In Booth’s view, the extreme financial reward of being the first to drug a novel target is the only thing that justifies the brutal, slow, and expensive process of uncovering new biology. When companies choose instead to join a “therapeutic crowd,” they are actively trading the steep scientific risks of unmapped biology for the intense commercial and clinical trial risks of a hyper-competitive market.
So, how did Vega Therapeutics pull off the impossible improbable? Despite generating robust proof-of-concept data, Vega Therapeutics is still the only company with a drug in clinical development specifically targeting Protein S for von Willebrand disease (VWD) as of June 2026.
For decades, VWD was viewed strictly through the lens of VWF replacement. In April 1924, a Finnish physician named Erik Adolf von Willebrand was consulted about a five-year-old girl named Hjördis Sundblom, who lived on a remote island in the Åland archipelago between Sweden and Finland. Upon investigation, Dr. von Willebrand mapped her family pedigree and discovered a terrifying hereditary pattern: 6 of her 10 siblings suffered from the same bleeding condition, and three of her sisters had already bled to death (tragically, Hjördis herself would later bleed to death at age 14 during her fourth menstrual period). In 1926, von Willebrand published his landmark paper, Hereditär pseudohemofili (”Hereditary Pseudohemophilia”).
In the 1950s, researchers in Sweden discovered that plasma from healthy individuals contained a mysterious “plasma factor” that could correct the bleeding time in Åland islanders. By the 1970s and 1980s, this massive glycoprotein was officially isolated, cloned, and named von Willebrand Factor (VWF). Scientists realized VWF plays two indispensable roles in normal hemostasis:
When a blood vessel is damaged, VWF acts as molecular double-sided tape. It binds to the exposed subendothelial collagen on one side and hooks onto the receptors (GPIb) of passing platelets on the other, forcing them to stop and form a plug.
In circulation, VWF binds to Factor VIII (the clotting factor missing in Hemophilia A), stabilizing it and protecting it from rapid degradation.
Today, VWD is recognized as the most common inherited bleeding disorder in humans, categorized into Type 1 (partial quantitative deficiency), Type 2 (qualitative/functional defects), and Type 3 (near-total absence of VWF, which is what Hjördis Sundblom suffered from).
Separately in 1977, pediatric hematologist Richard DiScipio and his colleagues first isolated and characterized Protein S but it was mistakenly pigeonholed as an anti-coagulant that acted independently of VWF for more than thirty years. The first cracks in this siloed view began to appear in the late 2000s and early 2010s, as vascular biologists began utilizing advanced microfluidic chambers that could simulate the immense mechanical forces inside living blood vessels. Scientists knew that VWF was a massive, tightly coiled polymer composed of over 40 to 100 linked monopers. Under normal, lazy blood flow, it drifted along like a crumpled ball of yarn. But when a blood vessel was ruptured, the local blood flow became turbulent and incredibly fast, a state known as high shear stress. This mechanical force literally yanked the VWF molecule open, unraveling it into long, sticky, linear strands. This highly specific, deeply hidden domain that acted like a molecular magnet for Protein S. The evolutionary elegance of this “molecular kidnapping” was breathtaking: by localizing and neutralizing the anti-coagulant brake (Protein S) exactly where the injury occurred, VWF allowed a localized explosion of thrombin generation.
This discovery re-wrote the pathology of von Willebrand disease. For a century, scientists believed that VWD patients bled simply because they lacked the duct tape to catch platelets. Now, they realized VWD was actually a catastrophic double-whammy. The patient lacked functional VWF, so platelets couldn’t anchor to the damaged blood vessel wall. Since there was no VWF to unravel and kidnap Protein S, the local injury site was flooded with unchecked, free-floating Protein S. The biological “brakes” were being slammed down completely wide open at the exact moment the body desperately needed to accelerate clotting.
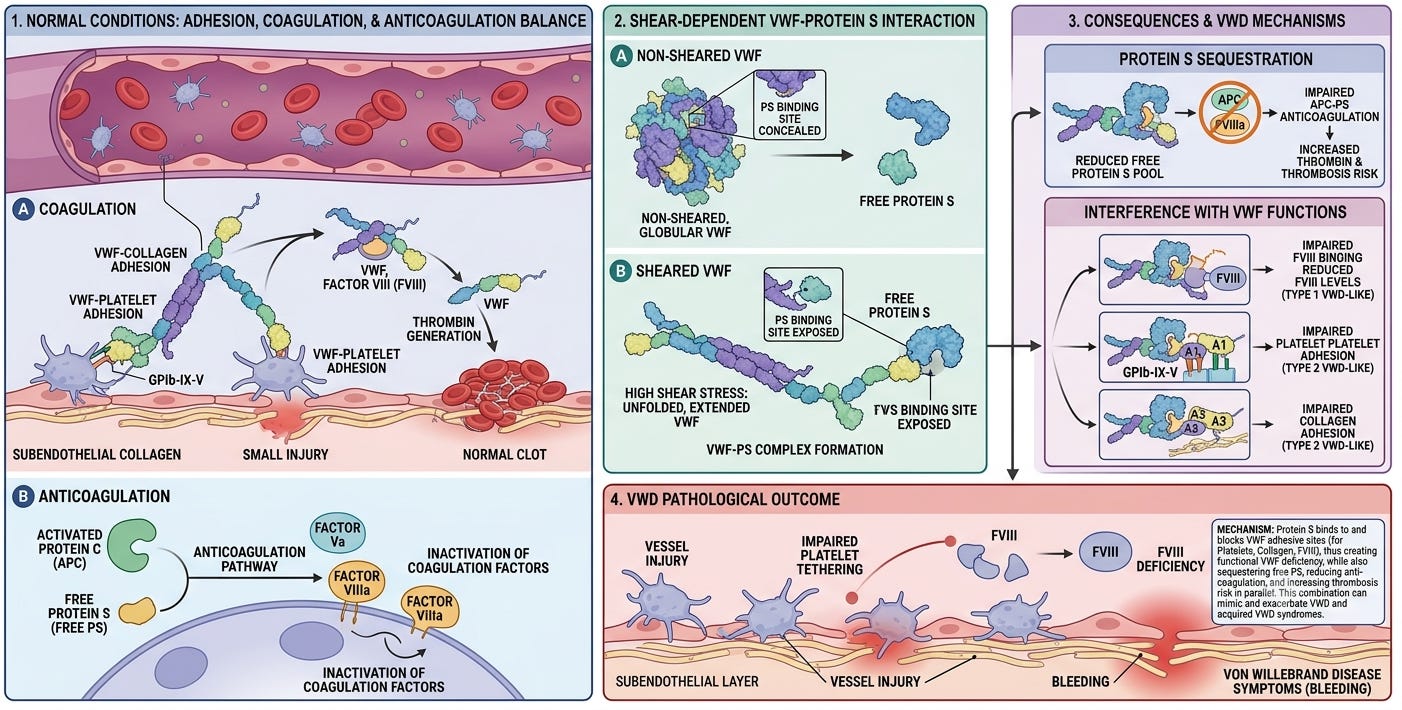
By 2018, academic proof-of-concept papers began floating an audacious hypothesis: if a VWD patient is suffering because free Protein S is suppressing their clotting capacity, what happens if we inhibit Protein S? This was the intellectual spark that ignited Star Therapeutics. Their drug hunters realized that trying to synthetically replace massive, fragile VWF molecules via lifelong intravenous infusions was an uphill battle. They engineered VGA039, a monoclonal antibody designed to bind to Protein S and block its ability to interact with its anti-coagulant partners, TFPI and APC, mimicking the role of VWF under shear stress. When Vega Therapeutics took this molecule into human trials in the early 2020s, the narrative came full circle. By deliberately disabling the Protein S brake, the drug allowed the coagulation cascade to generate robust, stable fibrin plugs entirely on its own. The body no longer needed VWF to sequester the brake because the drug had already neutralized it. When Vega presented its stunning multi-dose data at the ASH annual meeting in December 2025, showing up to a 100% reduction in annualized bleeding rates, they beat the odds and vaulted over the chasm of death between basic biology and translational drug discovery.
Conclusion
The story of Vega Therapeutics is both a massive financial win for Star Therapeutics and a high-impact proof of concept for the future of drug development. In an industry where capital naturally retreats to the relative safety of therapeutic crowding, Vega’s journey proves that the steep risks of unmapped biology can still yield the highest rewards. By transforming an elegant physiological insight into a Phase 3 asset, Vega has the potential to rewrite the standard of care for how we treat bleeding disorders. By daring to look away from crowded targets and zeroing in on the nuanced mechanics of Protein S, Vega demonstrated the viability of a completely novel therapeutic approach for patients with von Willebrand disease (VWD). As VGA039 transitions into Incyte’s commercial engine, it leaves behind a rich legacy of translating basic biology for the next generation of drug hunters and for Star Therapeutics’ other spokes.
To contact us, please send us an email at biotechreadout@gmail.com
Disclaimers
Investigational Status Disclaimer
The therapeutic candidates discussed in this newsletter are currently in clinical development and have not been approved for commercial sale by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), or other global regulatory authorities. Their safety and efficacy have not been established. References to pipeline products and ongoing clinical trials involve significant risks and uncertainties. Statements regarding the potential safety, potency, or efficacy of investigational drugs reflect current hypotheses and are not a guarantee of future performance or regulatory clearance. The outcome of clinical trials is inherently unpredictable, and clinical results from earlier stages may not be predictive of results in later, larger-scale trials.
No Medical Advice Disclaimer
This newsletter is for informational and educational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this publication.
No Patient-Provider Relationship Disclaimer
The information provided in this newsletter is for educational and analytical purposes only. Receipt of this information, or any interaction with this content, does not create a physician-patient, pharmacist-patient, or any other professional-provider relationship between you and the authors or publishers. This newsletter should not be used as a substitute for a personal consultation with a qualified healthcare professional.
Forward-Looking Statements Disclaimer
This newsletter contains “forward-looking statements” regarding future events, including clinical trial timing, regulatory milestones, and projected market performance. These statements are based on current expectations and assumptions that are subject to significant risks and uncertainties. Actual results may differ materially from those expressed or implied. We undertake no obligation to update these statements as a result of new information or future developments.
Third-Party Links & Content Disclaimer
This newsletter contains links to third-party websites, including clinical trial registries and corporate presentations. Biotech Readout does not endorse, guarantee, or assume responsibility for the accuracy or reliability of any information offered by third-party providers.
Errors and Omissions Disclaimer
While we strive for technical accuracy, the information in this newsletter is provided on an “as is” basis with no guarantees of completeness, accuracy, or timeliness. Biotech Readout assumes no liability for any errors or omissions in the content of this publication.
Non-Endorsement Disclaimer
Any reference to specific commercial products, processes, or services by trade name, trademark, or manufacturer does not constitute or imply an endorsement or recommendation by the author. All trademarks are the property of their respective owners.
No Investment Advice Disclaimer
This newsletter is for informational purposes only and does not constitute financial, investment, or legal advice. The author is not a registered investment advisor. You should consult with a professional financial advisor before making any investment decisions. The biotechnology sector is highly volatile; past performance is not indicative of future results.
Conflict of Interest Disclaimer
The author of this newsletter maintains a position of independence. At the time of publication, the author holds no direct financial interest, equity, or options in any of the companies mentioned in this report. No compensation has been received from any third party to feature or analyze specific therapeutic candidates or corporate entities.