
Eli Lilly to Acquire Vaccine with a Neurological Twist
Re-entering the vaccine market with multiple sclerosis (MS) upside

Disclaimer: This newsletter is for educational and informational purposes only and does not constitute medical, investment, or financial advice, nor does it establish a provider-patient relationship. Content may include forward-looking statements and discussions of investigational therapeutic candidates that are not FDA/EMA approved; their safety and efficacy remain unestablished and clinical outcomes are unpredictable. While we strive for accuracy, all information is provided as is without guarantees. This newsletter is independent, and the author holds no financial positions in the companies mentioned nor receives third-party compensation for this coverage. Please find a complete version of our disclaimers at the bottom of this article and on our About page.

Introduction
On May 26, 2026, Eli Lilly announced a definitive agreement to acquire three vaccine companies:
Curevo for up to $1.5 billion in cash, inclusive of an upfront payment and subsequent payment upon achievement of a specified milestone. Curevo’s lead program is amezosvatein (also known as CRV-101), a next-generation vaccine candidate designed to prevent shingles (herpes zoster) in adults. As of May 2026, the program is considered Phase 3-ready following the completion of a head-to-head Phase 2 trial against the current standard of care (Shingrix) in which amezosvatein met its primary endpoints, with reported data indicating a non-inferior humoral immune response in the evaluated cohort. Curevo leverages next-generation synthetic adjuvants aimed at matching standard-of-care efficacy while potentially addressing the “tolerability wall” that currently limits adult immunization.
LimmaTech Biologics for up to $780 million in cash, inclusive of an upfront payment and additional potential payments based upon the achievement of certain clinical and regulatory milestones. LimmaTech Biologics’ lead program is LTB-SA7, a vaccine candidate currently in Phase 1 development. The vaccine is designed to prevent infections caused by Staphylococcus aureus (S. aureus), which literature cites as a leading cause of surgical-site infections. LimmaTech leverages a “self-adjuvating” platform that shifts focus from mutable surface antigens to the stable toxins and superantigens that drive bacterial virulence, particularly in antibiotic-resistant environments.
Vaccine Company for up to $1.55 billion in cash, inclusive of an upfront payment and subsequent payments upon achievement of certain clinical and commercial milestones. Vaccine Company’s lead program is a five-antigen vaccine candidate targeting the Epstein-Barr Virus (EBV). As of May 2026, the program is “Phase 1-ready”. This company has developed a In Vivo Nanoparticles (IVN) platform combining the multivalent display of Virus-Like Particles (VLPs) with the manufacturing efficiency of modern delivery systems, bypassing traditional VLP production bottlenecks.
The “infectious disease legacy” that Eli Lilly mentioned in their press release might allude to their role as the primary industrial partner to manufacture and distribute the Jonas Salk’s polio vaccine in 1955. Nevertheless, Eli Lilly does not have an active, human commercial vaccine portfolio as of May 2026, so these acquisitions get them back in the game.
While each of these companies are impressive in their own ways, with compelling lead products and complimentary platforms, I want to focus on Vaccine Company, which is particularly interesting in two ways: its connection with multiple sclerosis, and its acquisition price.
The MS Mystery
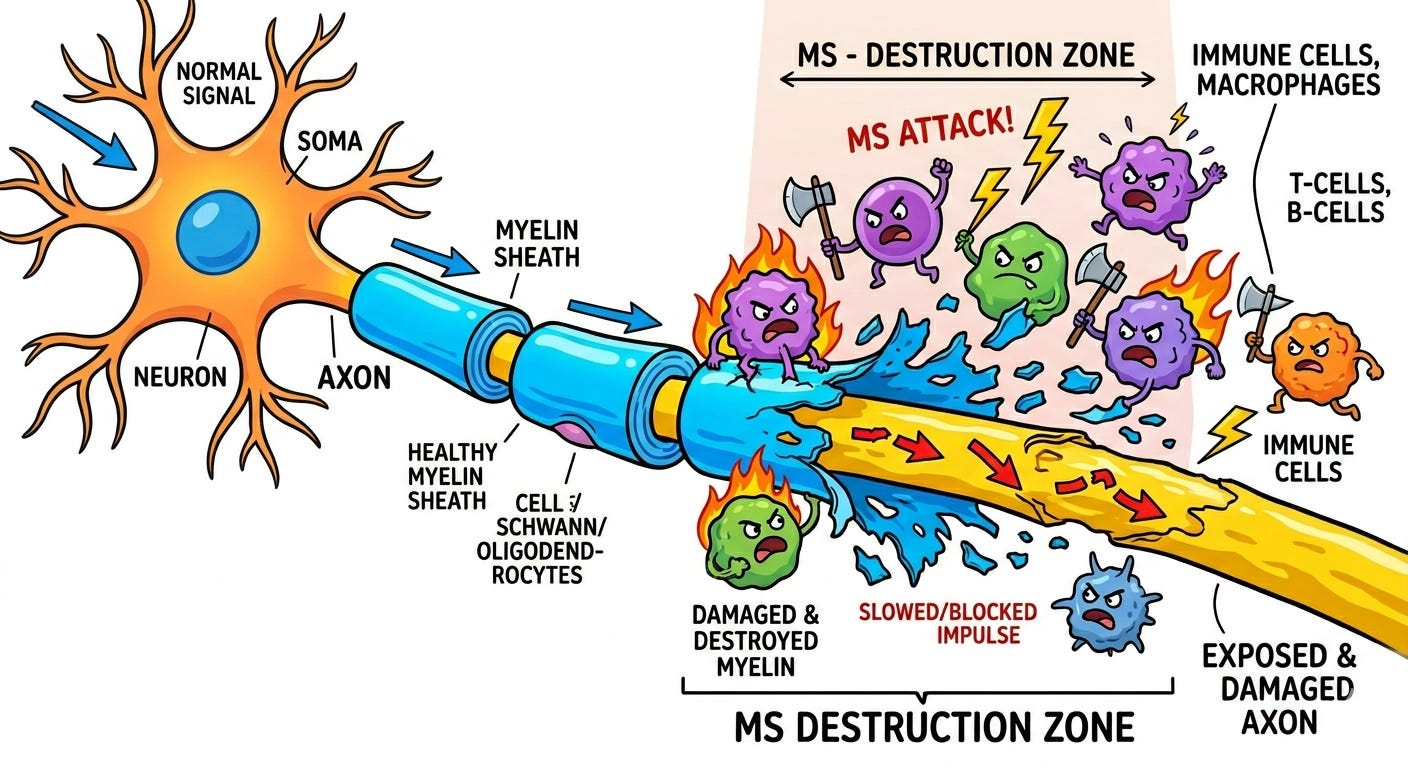
Multiple Sclerosis (MS) is a chronic, immune-mediated disease of the central nervous system (CNS) characterized by a misguided autoimmune attack against myelin, the protective sheath surrounding nerve fibers. In genetically susceptible individuals, environmental triggers cause peripheral T-cells and B-cells to breach the blood-brain barrier. Once inside the CNS, these activated immune cells orchestrate a cascade of inflammation, releasing pro-inflammatory cytokines and recruiting macrophages that actively destroy myelin and oligodendrocytes (the myelin-producing cells). This demyelination disrupts the saltatory conduction of action potentials, slowing or blocking nerve signals. Over time, the loss of trophic support from myelin, combined with direct oxidative stress and excitotoxicity, leads to irreversible axonal transection and neurodegeneration, manifesting as focal lesions (plaques) visible on neuroimaging and resulting in progressive neurological deficit.
So, why am I rambling about multiple sclerosis (MS) and what does it have to do with infectious disease? For decades, Multiple Sclerosis (MS) was categorized as a neurological mystery of “unknown etiology.” However, recent landmark longitudinal data and molecular breakthroughs have provided what is now considered an etiological hallmark: the Epstein-Barr Virus (EBV) could very well be the leading cause of MS. This discovery dramatically shifts our clinical perspective, moving MS from a condition of inevitable nerve degeneration to a primary target for preventative vaccines.
Historically, there were subtle clues that EBV might play a role in MS. EBV is incredibly common, infecting roughly 95% of all adults globally. However, MS is a relatively rare neurological disease. If the link was credible, the clinical onset of MS symptoms would have to occur a decade or more after the initial EBV infection. To establish a link, researchers needed a massive, longitudinal study that tracked EBV-negative individuals over many years to see if acquiring the virus preceded the onset of MS. That study arrived in a 2022 paper in Science titled “Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis”.
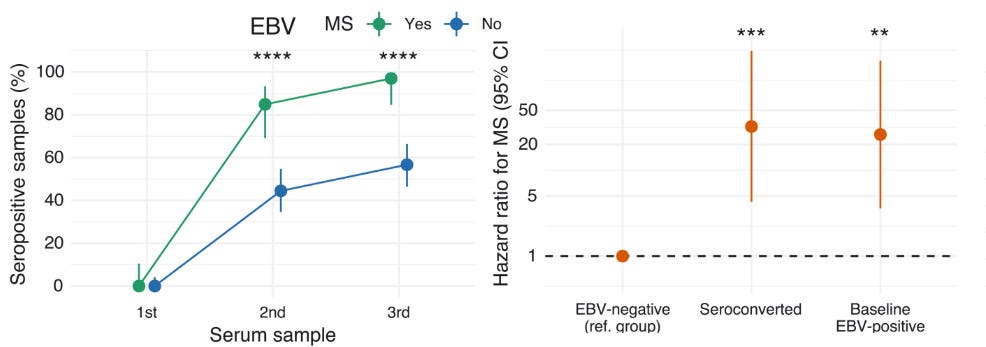
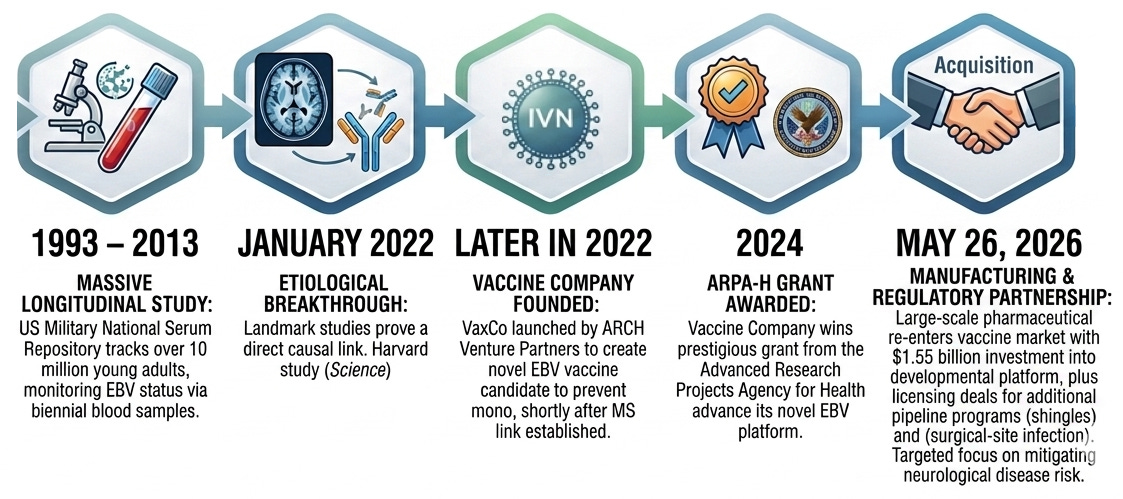
The research team, led by scientists at the Harvard T.H. Chan School of Public Health, utilized a unique data source: The US Military National Serum Repository. They tracked a cohort of more than 10 million young adults on active duty in the US military between 1993 and 2013. The military takes biennial (every two years) blood samples from service members. The researchers analyzed these stored serum samples to check the soldiers’ EBV status over time. Within this multi-million person cohort, they identified 955 individuals who were diagnosed with MS during their period of military service.
The researchers looked closely at individuals who were EBV-negative when they first entered the military. Out of those who later developed MS, all but one individual seroconverted (tested positive for EBV) prior to their MS diagnosis. They found that the risk of developing MS increased 32-fold after individuals became infected with EBV. To put this in perspective, this magnitude of effect is remarkably high, comparable to the correlation between heavy smoking and lung cancer (15-30 fold increased risk according to CDC). In contrast, infection with CMV (a different virus thought to be present in >50% of people ≥40 years old) showed no increase in MS risk. The team measured serum levels of neurofilament light chain (sNfL), a well-established blood biomarker that spikes when nerve cells in the brain and spinal cord are damaged or degenerating. They found that sNfL levels only began to rise after EBV infection.
While these findings implied a causal link between EBV and MS, there remained a glaring hole in our understanding: how exactly does EBV drive neurodegeneration? We didn’t have to wait very long for the answer. A mere 11 days after the Harvard team published their massive epidemiological study, a team at Stanford published a paper in Nature that expanded on the mechanistic link between EBV and MS.
In MS, B cells gather in the cerebrospinal fluid (CSF) and secrete abnormal antibodies (visible on diagnostic tests as “oligoclonal bands”). The team set out to map the genetic sequences of these specific B cells to determine exactly what targets those antibodies were mistakenly attacking. The team utilized a sophisticated multi-step approach.
Single-Cell Sequencing: They isolated B cells and antibody-secreting plasmablasts directly from the blood and CSF of patients with Relapsing-Remitting MS (RRMS). They sequenced the paired heavy- and light-chain B-cell receptors (BCRs) to recreate the exact antibodies being produced in the central nervous system.
Recombinant Expression: They structurally recreated these human antibodies in the lab.
Microarray Screening: They ran these recreated MS antibodies against broad protein microarrays containing thousands of both human proteins and viral proteins (including MS-associated herpesviruses) to see what they would bind to.
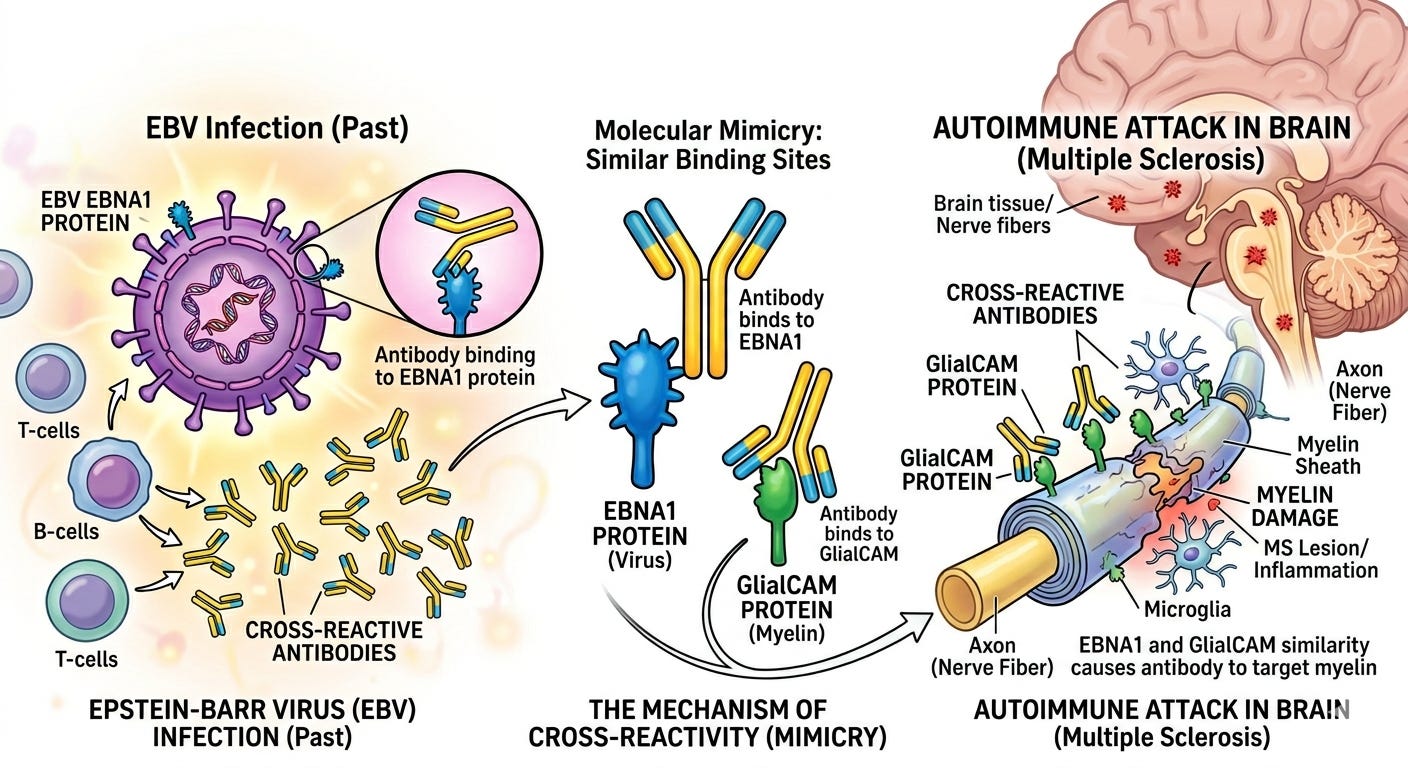
The microarrays revealed that monoclonal antibodies from several MS patients reacted strongly to EBNA1 (Epstein-Barr virus nuclear antigen 1), a critical transcription factor the virus uses during its latent phase. Crucially, one specific high-affinity, CSF-derived antibody (labeled MS39p2w174) bound tightly to an epitope on EBNA1, but also cross-reacted with a human central nervous system protein called GlialCAM (glial cell adhesion molecule).
This cross-reactivity is a prime example of molecular mimicry, where a piece of a foreign pathogen looks so similar to a self-protein that the immune system gets confused. The researchers solved the 2.5 Å resolution crystal structure of the antibody bound to the EBV peptide. They discovered that the antibody binds a specific proline/arginine-rich loop. The molecular mimicry is uniquely facilitated by a post-translational modification. When GlialCAM is phosphorylated at the Ser376 residue (a normal cellular process in the brain), its structural resemblance to the EBV EBNA1 protein becomes even stronger, locking the cross-reactive antibodies onto glial cells with incredibly high affinity.
To prove this mimicry actually drives disease rather than just being an accidental bystander effect, the team immunized mouse models of MS (Experimental Autoimmune Encephalomyelitis, or EAE) with the EBV EBNA1 protein. The EBNA1 immunization severely exacerbated the disease, causing increased trafficking of immune cells into the central nervous system and accelerating demyelination. When testing broader patient cohorts, they discovered that elevated levels of anti-EBNA1 and anti-GlialCAM antibodies were highly prevalent in patients with MS compared to healthy controls, validating that this mechanism is a widespread feature of the disease.
While epidemiologists had proven that Epstein-Barr virus (EBV) causes multiple sclerosis (MS) risk to skyrocket, Lanz et al. provided the precise, definitive mechanistic smoking gun explaining that the virus stimulates pathogenic cross-reactive antibodies that triggers an anti-EBV response by binding EBNA1, but an unintended anti-myelin response by binding GlialCAM.
Premium Preclinical
Capital is following the science. Eli Lilly’s acquisition of Vaccine Company could give them a candidate for potentially combatting EBV and multiple sclerosis (MS), although the lead program is currently Phase 1-ready and has not yet entered clinical trials. In this vein, Daniel M. Skovronsky, M.D., Ph.D., chief scientific and product officer, and president, Lilly Research Laboratories commented, “decades of evidence now link common infections to diseases that potentially emerge years later, including neurological disease […] combining these companies’ platforms and teams with Lilly’s global scale positions us to change that trajectory.” Perhaps that partially accounts for the company’s substantial acquisition price of up to $1.55 billion, which represents a premium relative to historical average takeout prices for preclinical companies in recent cohorts (about $600 million, n=22). Or perhaps there are multiple compounding variables at play.
Vaccine Company (often stylized as VaxCo) was founded in 2022 by ARCH Venture Partners, one of the industry’s most prominent life sciences venture capital firms. ARCH launched the startup with a specific mission: to disrupt traditional vaccine design by bringing next-generation antigen engineering and advanced manufacturing to vaccine science. The company’s primary asset is its proprietary in vivo nanoparticle (IVN) technology platform. The IVN platform is designed to ease and streamline the complex manufacturing processes traditionally required to produce virus-like particle (VLP) vaccines. VLPs mimic the physical structure of native viruses to trigger a potent immune response without containing actual viral genetic material. Vaccine Company’s platform optimized how these structural proteins are engineered, aiming to offer a more scalable, high-yield path toward commercial production.
While many vaccine startups focused heavily on mRNA applications for respiratory illnesses, Vaccine Company differentiated itself by tackling massive, unmet public health crises linked to latent viral infections. The team nominated a lead candidate designed to prevent infectious mononucleosis caused by the Epstein-Barr virus (EBV), a choice made shortly after the epidemiologic and mechanistic links were established with multiple sclerosis (MS) in January of 2022. In 2024, the company’s novel approach earned a highly competitive grant from ARPA-H (the Advanced Research Projects Agency for Health).
Taken together, a number of factors could account for Vaccine Company’s acquisition premium including smart and timely indication selection, strong institutional backing, and a novel platform.
Conclusion
The journey from the US Military Serum Repository to a $1.55 billion acquisition platform highlights the remarkable speed of modern biotechnology when capital follows ironclad science. In less than four years, the industry has gone from epidemiologically showing that EBV drives MS, to mapping the exact molecular mimicry of GlialCAM, to a major pharmaceutical player acquiring an asset that aims to address the disease at their root cause. Eli Lilly’s newly acquired infectious disease pipeline has given the market a fascinating neurological twist and could give patients hope of a future where multiple sclerosis is rarer than it already is.
To contact us, please send us an email at biotechreadout@gmail.com
Disclaimers
Investigational Status Disclaimer
The therapeutic candidates discussed in this newsletter are currently in clinical development and have not been approved for commercial sale by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), or other global regulatory authorities. Their safety and efficacy have not been established. References to pipeline products and ongoing clinical trials involve significant risks and uncertainties. Statements regarding the potential safety, potency, or efficacy of investigational drugs reflect current hypotheses and are not a guarantee of future performance or regulatory clearance. The outcome of clinical trials is inherently unpredictable, and clinical results from earlier stages may not be predictive of results in later, larger-scale trials.
No Medical Advice Disclaimer
This newsletter is for informational and educational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this publication.
No Patient-Provider Relationship Disclaimer
The information provided in this newsletter is for educational and analytical purposes only. Receipt of this information, or any interaction with this content, does not create a physician-patient, pharmacist-patient, or any other professional-provider relationship between you and the authors or publishers. This newsletter should not be used as a substitute for a personal consultation with a qualified healthcare professional.
Forward-Looking Statements Disclaimer
This newsletter contains “forward-looking statements” regarding future events, including clinical trial timing, regulatory milestones, and projected market performance. These statements are based on current expectations and assumptions that are subject to significant risks and uncertainties. Actual results may differ materially from those expressed or implied. We undertake no obligation to update these statements as a result of new information or future developments.
Third-Party Links & Content Disclaimer
This newsletter contains links to third-party websites, including clinical trial registries and corporate presentations. Biotech Readout does not endorse, guarantee, or assume responsibility for the accuracy or reliability of any information offered by third-party providers.
Errors and Omissions Disclaimer
While we strive for technical accuracy, the information in this newsletter is provided on an “as is” basis with no guarantees of completeness, accuracy, or timeliness. Biotech Readout assumes no liability for any errors or omissions in the content of this publication.
Non-Endorsement Disclaimer
Any reference to specific commercial products, processes, or services by trade name, trademark, or manufacturer does not constitute or imply an endorsement or recommendation by the author. All trademarks are the property of their respective owners.
No Investment Advice Disclaimer
This newsletter is for informational purposes only and does not constitute financial, investment, or legal advice. The author is not a registered investment advisor. You should consult with a professional financial advisor before making any investment decisions. The biotechnology sector is highly volatile; past performance is not indicative of future results.
Conflict of Interest Disclaimer
The author of this newsletter maintains a position of independence. At the time of publication, the author holds no direct financial interest, equity, or options in any of the companies mentioned in this report. No compensation has been received from any third party to feature or analyze specific therapeutic candidates or corporate entities.