
Eli Lilly to Acquire Kelonia
Digging into the in vivo CAR-T gold rush

Disclaimer: This newsletter is for educational and informational purposes only and does not constitute medical, investment, or financial advice, nor does it establish a provider-patient relationship. Content may include forward-looking statements and discussions of investigational therapeutic candidates that are not FDA/EMA approved; their safety and efficacy remain unestablished and clinical outcomes are unpredictable. While we strive for accuracy, all information is provided as is without guarantees. This newsletter is independent, and the author holds no financial positions in the companies mentioned nor receives third-party compensation for this coverage. Please find a complete version of our disclaimers at the bottom of this article and on our About page.

Introduction
On April 20, 2026, Eli Lilly and Company announced a definitive agreement to acquire Kelonia Therapeutics up to $7.00 billion in cash, inclusive of an upfront payment of $3.25 billion, and subsequent payments upon achievement of certain clinical, regulatory and commercial milestones. This acquisition centers on Kelonia’s iGPS platform, a specialized delivery system that modifies a patient’s T-cells directly inside the body to fight cancer (“in vivo CAR-T”). Unlike traditional CAR-T therapies that require complex external manufacturing and harsh chemotherapy, Kelonia’s approach is designed to offer a simpler, off-the-shelf alternative, pending further clinical validation and regulatory review. Initial clinical data for the lead candidate, KLN-1010, showed an overall response rate of 100% in a limited cohort of four patients with multiple myeloma. Jacob Van Naarden, executive vice president and president of Lilly Oncology and head of corporate business development, commented, “Autologous CAR-T therapies have meaningfully improved outcomes for patients with various cancers, but significant manufacturing, safety, and access hurdles mean that only a fraction of eligible patients actually receive them. Kelonia’s in vivo platform has the potential to change that by delivering rapid, durable responses in a far simpler, off-the-shelf format.”
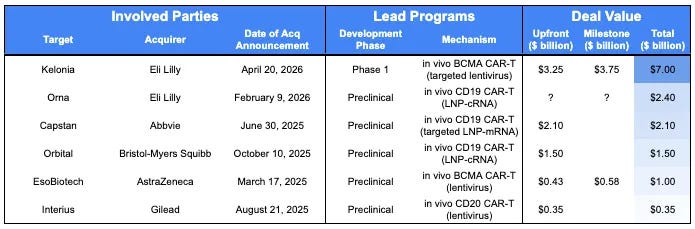
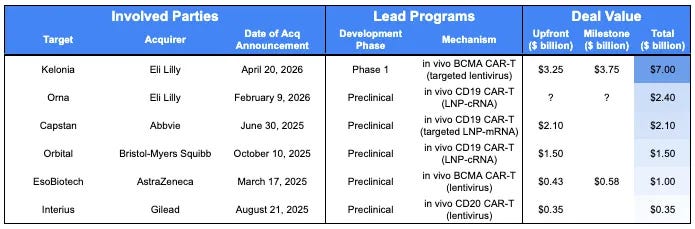
Recent acquisitions of in vivo CAR-T companies have been unusual:
High Volume of Deals: There have been six acquisitions involving these technologies in past 13 months, which is an unusually high cadence.
Early Stage of Deals: Typically, pharmaceutical companies prefer to acquire FDA-approved or Phase 3 assets (~61% of acquisitions in our internal dataset) because they generate a better risk-adjusted return on investment, a must-have in order to compensate for impending patent cliffs. In contrast, most in vivo CAR-T acquisitions have been for preclinical-stage assets, with Kelonia being the only exception (Phase 1 data but only in four patients).
Here, we expand on how in vivo approaches advance the cutting edge and speculate on the factors driving acquirer conviction at the earliest stages of validation.
Optional Detour: The History of CAR-T
We covered the history of CAR-T in Part 1 of our CAR-T series here. You are more than welcome to check it out if you’re interested in learning about the Immunology Civil War, the discovery of T-cells, and their rebirth as medicines. Make sure to return to this piece afterwards to learn more about the Eli Lilly-Kelonia acquisition!
Or, feel free to continue reading if you are specifically interested in the Eli Lilly-Kelonia acquisition.
CAR-T Goes In Vivo
Our journey from the discovery of CAR-T, and discussion of the various challenges that limit access and adds treatment burden (ie. month-long manufacturing/cold chain and lymphodepleting chemotherapy) brings us back to the acquisition of Kelonia Therapeutics. How are is their technology different, and how do the advance the cutting edge of CAR-T therapy?
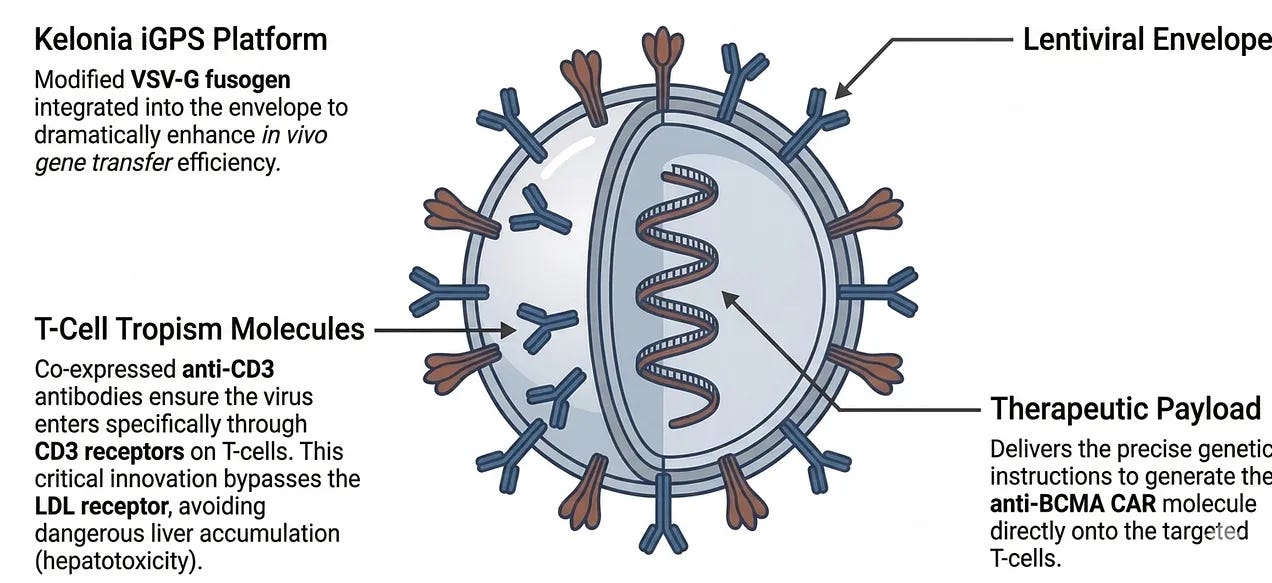
Kelonia’s iGPS platform (in vivo Gene Placement System) is designed to turn a patient’s own body into a factory for CAR-T cells. Instead of the complex process of removing a patient’s cells for laboratory modification, the iGPS therapy is administered as a single, direct intravenous infusion. The treatment uses specially engineered particles (modified lentiviruses) that are designed to selectively find and enter T-cells already circulating in the patient’s bloodstream. Once these particles enter the T-cells, they are designed to deliver genetic instructions that program those cells to become CAR-T cells. These newly created CAR-T cells then multiply and begin seeking out and destroying cancer cells throughout the body.
Eli Lilly’s stated rationale for the acquisition highlights the platform’s potential to democratize therapy by removing the vein-to-vein times and complex manufacturing cycles of traditional autologous CAR-T. By shifting the manufacturing site to the patient’s own body, the in vivo Gene Placement System (iGPS) platform provides an off-the-shelf solution that can be administered via standard intravenous infusion, with the intended goal of potentially enabling treatment in community-based settings, pending regulatory review of its safety profile in non-academic environments. The iGPS platform relies on three foundational technical pillars:
Vector Architecture: The platform utilizes an advanced, third-generation lentiviral vector (LVV). Critically, because T-cells are proliferating cells, the integrating nature of LVV provides a significant advantage over non-integrating RNA modalities; the genetic payload remains stable as the cells divide, ensuring superior therapeutic durability.
Targeting Mechanism: To avoid the liver accumulation common in systemic delivery, iGPS utilizes a modified vesicular stomatitis virus glycoprotein (VSV-G) fusogen co-expressed with an anti-CD3 antibody on the lentiviral envelope. This ensures viral entry is facilitated specifically through CD3 on T-cells, rather than the low-density lipoprotein receptor (LDLR) used by standard VSV-G. This mechanism is designed to mitigate non-specific liver uptake, a primary safety hurdle for competing lipid nanoparticle (LNP) technologies.
Therapeutic Delivery: The system facilitates the generation of CAR-T cells directly in the circulation through a single infusion, eliminating the need for apheresis and the toxic lymphodepleting chemotherapy regimens required for ex vivo engraftment. Unlike non-integrating technologies such as mRNA or circular RNA, iGPS’ integrating lentiviral vector ensures the CAR transgene is maintained through T-cell proliferation and differentiation, providing a stable genetic modification essential for long-term surveillance.
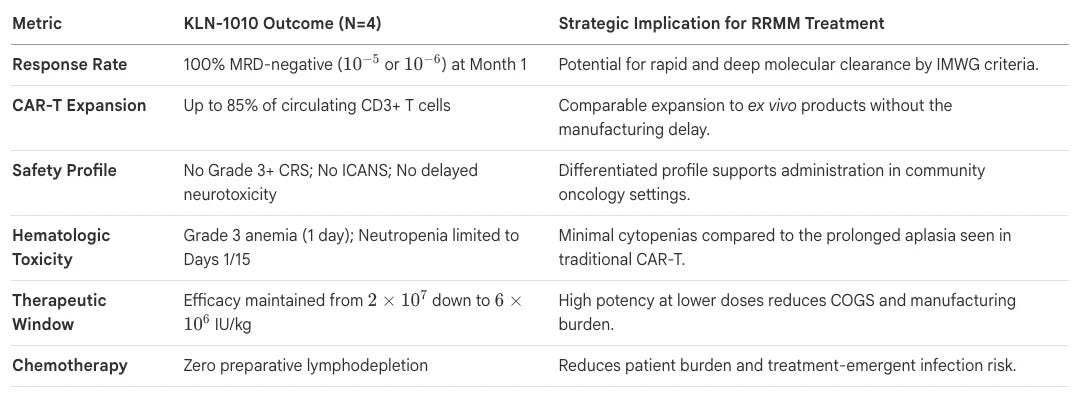
In the unproven and high-risk field of in vivo genetic medicine, early human data is the essential metric for de-risking multi-billion dollar capital outlays. Kelonia’s lead program, KLN-1010, has provided this validation through its Phase 1 inMMyCAR trial in relapsed/refractory multiple myeloma (r/r MM). Preliminary data presented at the America Society for Hematology (ASH) 2025 meeting for the initial four patients showed:
Efficacy: A 100% minimal residual disease (MRD)-negative response rate across four patients (ie. undetectable cancer in all treated patients); MRD-negative responses were maintained through three months in the two patients with the longest follow up. Three of the four patients were treated at 2×107 IU/kg. Deep responses and favorable safety profile compelled exploration of the therapeutic window to further reduce the cost of goods. The fourth patient was treated at a lower dose of 6×106 IU/kg and achieved an MRD-negative response at month 1. All four patients remain in response, per International Myeloma Working Group’s (IMWG) criteria, with the longest follow-up of five months; complete response (CR) was the best overall response.
Expansion and Durability: Robust CAR-T cell expansion similar to ex vivo therapies despite no lymphodepleting chemotherapy; reaching up to 85% of circulating T-cells. Persistent memory CAR-T in all patients observed through three months to date, which suggests KLN-1010 provides a reservoir for sustained anti-tumor surveillance. This integrates the rapid response of cellular therapy with the long-term control traditionally sought in vaccine or antibody-based approaches.
Safety: Favorable toxicity profile with no cytokine release syndrome (CRS) of grade 3 or above, no Immune Effector Cell-Associated Neurotoxicity Syndrome (ICANS), no delayed neurotoxicity, and markedly lower cytopenias compared to ex vivo CAR-T cell therapies.
In Vivo CAR-T Gold Rush Starts with the First Nugget
The Kelonia-Eli Lilly transaction highlights a remarkably efficient capital model. Originally incubated and seed funded by Venrock, Kelonia raised only $60 million in total private capital. For Venrock, the $20 million seed investment yields a $900 million return on the upfront payment alone (~45x), with the potential for a 100x return upon achievement of the $7 billion milestone total.
The story of Kelonia Therapeutics was a classic lab-to-launch biotech narrative. The scientific foundation of Kelonia was built at the Massachusetts Institute of Technology (MIT). The company’s technology is based on research from the laboratory of Dr. Michael Birnbaum, an Associate Professor of Biological Engineering. Dr. Birnbaum’s work focused on re-engineering viruses. While most gene therapy uses viral vectors to deliver genes, they are often clunky, they hit the wrong cells or aren’t efficient enough. Dr. Birnbaum and his team developed a way to create Lentiviral-like Particles (LVPs) that were essentially GPS-guided. By modifying the surface of these particles, they could ensure the genetic payload was only delivered to specific cells (like T-cells) while they were still inside the body.
Recognizing the commercial potential of an in vivo (inside the body) delivery system, the venture capital firm Venrock incubated the company. Kelonia officially launched in April 2022 with a $50 million Series A funding round. The company was led by Dr. Kevin Friedman, a veteran of the cell therapy space who had previously played a key role at bluebird bio and 2seventy bio. From day one, the company’s “North Star” was to eliminate the need for the multi-week, multi-hundred-thousand-dollar manufacturing process required for traditional CAR-T.
Kelonia branded its core technology as the iGPS (In Vivo Gene Placement System). To prove it worked, they focused on Multiple Myeloma, targeting a protein called BCMA. Big Pharma noticed early. In 2024, Kelonia signed major collaboration deals with Astellas and Johnson & Johnson, signaling that the industry viewed their off-the-shelf approach as a serious threat to the status quo. The turning point for the company came in December 2025 at the American Society of Hematology (ASH) Annual Meeting, which we covered in the previous section.
The surge of in vivo CAR-T acquisitions in the past 13 months confirms that Big Pharma is interested in moving away from the vein-to-vein logistics of the past. For the Eli Lilly team, the acquisition of Kelonia could be rooted in a diversification approach, recognizing that no single delivery vehicle will solve all in vivo CAR-T challenges. This puts the Kelonia acquisition at the forefront of an industry-wide spend exceeding $5 billion, alongside peers such as AbbVie, AstraZeneca, and Bristol-Myers Squibb.
While all such approaches are early-stage, the field is quickly becoming crowded. Kelonia serves as a complementary, rather than redundant, asset to Eli Lilly’s recent acquisition of Orna Therapeutics in three main ways:
Modality & Maturity: Kelonia utilizes an integrating lentiviral approach, already validated in refractory patients (Phase 1). In contrast, Orna utilizes a non-integrating circular RNA (oRNA) delivered via LNPs, currently in Phase 1 with healthy volunteers.
Targeting & Disease Scope: Kelonia’s KLN-1010 focuses on anti-BCMA (Multiple Myeloma), while Orna’s ORN-252 targets anti-CD19 (B-cell cancers and autoimmune diseases).
Strategic Moat: Through this acquisition, Eli Lilly is positioned to assume Kelonia’s established strategic collaborations with Johnson & Johnson and Astellas. These agreements could provide Eli Lilly with oversight of partner-funded pipelines, subject to the terms and successful continuation of those specific development programs.
Owning both integrating (Kelonia) and non-integrating (Orna) platforms provides Eli Lilly with a diversified toolkit of genetic delivery mechanisms. They would be able to select the optimal modality based on whether a specific disease requires the permanent genetic modification afforded by LVV or the more transient effects of oRNA, helping to future-proof their oncology and immunology pipelines against competitive technological shifts.
Conclusion
The winner of the in vivo CAR-T race remains to be seen as pharmaceutical giants continue to place multi-billion dollar bets on these competing delivery mechanisms. Regardless of who leads the pack, the inevitable outcome is a more resilient and accessible arsenal for oncology. The ultimate victory will belong to the patients who finally gain access to these highly effective but once-elusive treatments.
To contact us, please send us an email at biotechreadout@gmail.com
Disclaimers
Investigational Status Disclaimer
The therapeutic candidates discussed in this newsletter are currently in clinical development and have not been approved for commercial sale by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), or other global regulatory authorities. Their safety and efficacy have not been established. References to pipeline products and ongoing clinical trials involve significant risks and uncertainties. Statements regarding the potential safety, potency, or efficacy of investigational drugs reflect current hypotheses and are not a guarantee of future performance or regulatory clearance. The outcome of clinical trials is inherently unpredictable, and clinical results from earlier stages may not be predictive of results in later, larger-scale trials.
No Medical Advice Disclaimer
This newsletter is for informational and educational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this publication.
No Patient-Provider Relationship Disclaimer
The information provided in this newsletter is for educational and analytical purposes only. Receipt of this information, or any interaction with this content, does not create a physician-patient, pharmacist-patient, or any other professional-provider relationship between you and the authors or publishers. This newsletter should not be used as a substitute for a personal consultation with a qualified healthcare professional.
Forward-Looking Statements Disclaimer
This newsletter contains “forward-looking statements” regarding future events, including clinical trial timing, regulatory milestones, and projected market performance. These statements are based on current expectations and assumptions that are subject to significant risks and uncertainties. Actual results may differ materially from those expressed or implied. We undertake no obligation to update these statements as a result of new information or future developments.
Third-Party Links & Content Disclaimer
This newsletter contains links to third-party websites, including clinical trial registries and corporate presentations. Biotech Readout does not endorse, guarantee, or assume responsibility for the accuracy or reliability of any information offered by third-party providers.
Errors and Omissions Disclaimer
While we strive for technical accuracy, the information in this newsletter is provided on an “as is” basis with no guarantees of completeness, accuracy, or timeliness. Biotech Readout assumes no liability for any errors or omissions in the content of this publication.
Non-Endorsement Disclaimer
Any reference to specific commercial products, processes, or services by trade name, trademark, or manufacturer does not constitute or imply an endorsement or recommendation by the author. All trademarks are the property of their respective owners.
No Investment Advice Disclaimer
This newsletter is for informational purposes only and does not constitute financial, investment, or legal advice. The author is not a registered investment advisor. You should consult with a professional financial advisor before making any investment decisions. The biotechnology sector is highly volatile; past performance is not indicative of future results.
Conflict of Interest Disclaimer
The author of this newsletter maintains a position of independence. At the time of publication, the author holds no direct financial interest, equity, or options in any of the companies mentioned in this report. No compensation has been received from any third party to feature or analyze specific therapeutic candidates or corporate entities.